Department of Thoracic Surgery, The Fourth Affiliated Hospital of China Medical University, 4 Chongshan East Road, Shenyang, 110032, Liaoning, People's Republic of China.
Acornmed Biotechnology Co., Ltd., 13 Kechuang Road, Beijing, 100176, People's Republic of China.
BMC Pulm Med. 2021 Apr 17;21(1):125. doi: 10.1186/s12890-021-01490-x.
The identification of NTRK fusions in tumours has become critically important due to the actionable events predictive of response to TRK inhibitor. It is not clear whether the NTRK breakpoint location is different for response to targeted therapy and NTRK fusions affects the efficacy of immunotherapy.
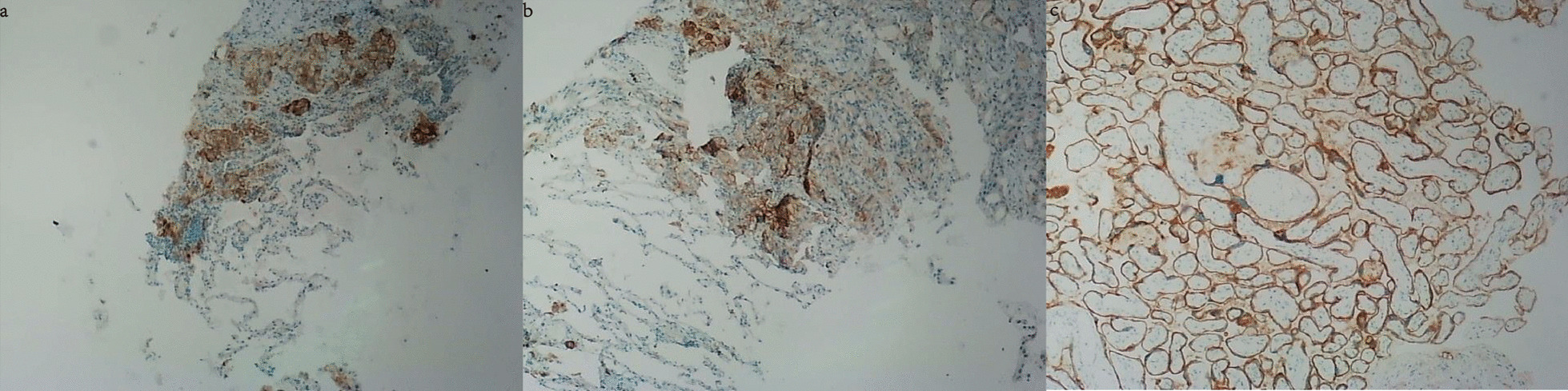
Here we reported a 60-year-old female diagnosed with advanced lung adenocarcinoma. NGS-based molecular profiling identified a novel NCOR2-NTRK1 fusion and high tumor mutational burden (TMB) (58.58 mutations/Mb) in this case. Additionally, program death-ligand 1 (PD-L1) expression was detected in 20-30% of the tumor cells by immunohistochemical (IHC) staining. The patient received treatment with anti-PD-1 immune checkpoint inhibitor of camrelizumab. After two cycles of treatment, the CT scan showed some tumor nodules were still enlarged, indicating disease progression. She was then changed to TRK inhibitor larotrectinib. One month later, the CT scan showed the volume of some lesions started to decrease, and no metastasis lesions were found. The patient then continued the administration of larotrectinib, and some lesion sizes were significantly reduced or even disappeared in the next few months. Currently, this patient is still alive.
Altogether, this report provided a new driver of lung adenocarcinoma expanded the mutational spectrum of NTRK1 fusion variants and suggested using larotrectinib as the targeted therapy is more effective than anti-PD-1 inhibitor in lung adenocarcinoma harboring with NTRK fusion, positive PD-L1 expression, and high TMB simultaneously.
由于预测对 TRK 抑制剂反应的可操作事件,肿瘤中 NTRK 融合的鉴定变得至关重要。目前尚不清楚 NTRK 断点位置是否因靶向治疗反应和 NTRK 融合而不同,以及是否会影响免疫疗法的疗效。
在这里,我们报告了一例 60 岁女性,被诊断为晚期肺腺癌。基于 NGS 的分子谱分析在该病例中发现了一种新型 NCOR2-NTRK1 融合和高肿瘤突变负担(TMB)(58.58 个突变/Mb)。此外,免疫组化(IHC)染色检测到 20-30%的肿瘤细胞中程序性死亡配体 1(PD-L1)表达。该患者接受了抗 PD-1 免疫检查点抑制剂 camrelizumab 的治疗。两个周期的治疗后,CT 扫描显示一些肿瘤结节仍在增大,表明疾病进展。随后,她改用 TRK 抑制剂 larotrectinib。一个月后,CT 扫描显示部分病变的体积开始减小,未发现转移病灶。随后,该患者继续接受 larotrectinib 治疗,在接下来的几个月中,一些病变的大小明显缩小甚至消失。目前,该患者仍存活。
总之,本报告提供了一种新的肺腺癌驱动基因,扩大了 NTRK1 融合变异体的突变谱,并提示在同时携带 NTRK 融合、PD-L1 阳性和高 TMB 的肺腺癌中,使用 larotrectinib 作为靶向治疗比抗 PD-1 抑制剂更有效。