EMD Serono Inc., Rockland, MA, USA; an affiliate of Merck KGaA, Darmstadt, Germany.
STATinMED Research, Plano, TX, USA.
Adv Ther. 2021 May;38(5):2644-2661. doi: 10.1007/s12325-021-01657-2. Epub 2021 Apr 17.
Substantial unmet needs exist among patients with metastatic renal cell carcinoma (mRCC). This retrospective study evaluated treatment patterns as well as clinical and economic outcomes associated with first-line monotherapy among patients with mRCC in the USA.
Newly diagnosed patients with mRCC initiating at least one first-line therapy (1L) from 1 October 2013 to 31 March 2018 (index date = 1L start date) were identified from the US Veterans Health Administration database. Treatment patterns, clinical outcomes (time to next treatment [TNT] defined by earliest of switch to non-index therapy or re-initiation of index therapy after a more than 90-day gap, time to treatment discontinuation [TTD], overall survival [OS]), and costs were evaluated among patients treated with tyrosine kinase inhibitors (TKI), mammalian target of rapamycin inhibitors (mTOR), immune checkpoint inhibitors (ICI), and other monotherapies. Standard descriptive statistics were presented. The Kaplan-Meier method was used to evaluate clinical outcomes.
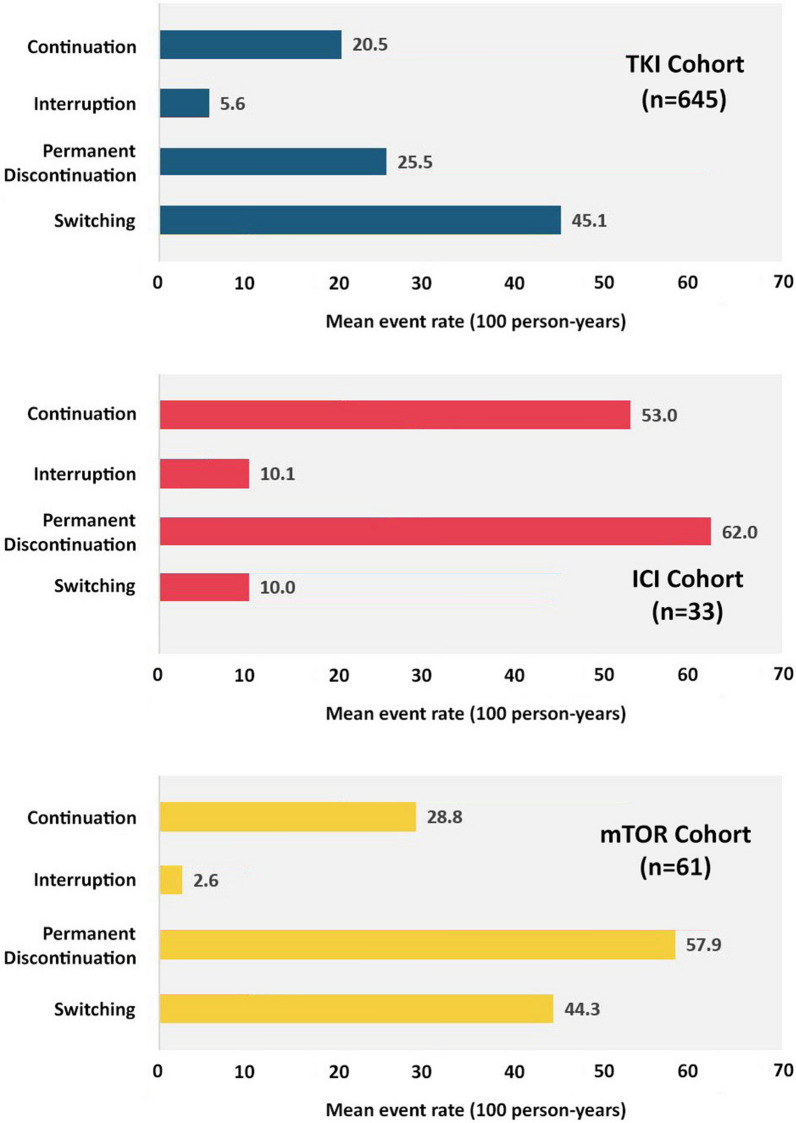
Of 759 patients (median age 68.0 years), 85.0%, 8.0%, 4.3%, and 2.6% were treated with TKI, mTOR, ICI, or other therapy in 1L, respectively. Advancement rates (to second-line [2L] therapy) ranged from 10.0 (ICI) to 45.1 per 100 person years (TKI). The 12-month OS rates ranged from 47.4% (TKI) to 67.7% (mTOR). The median TNT ranged from 3.8 (mTOR) to 9.6 months (ICI), and median TTD ranged from 2.3 (mTOR) to 4.7 months (TKI). Total all-cause mean costs per patient per month ranged from $12,466 (mTOR) to $19,812 (ICI).
These results indicate high unmet medical needs among patients with mRCC treated with 1L monotherapies. Novel combination therapies (e.g., ICI + ICI, ICI + TKI) may improve front-line outcomes for patients with poor prognoses.
转移性肾细胞癌(mRCC)患者存在大量未满足的需求。这项回顾性研究评估了美国 mRCC 患者一线单药治疗的治疗模式以及与一线单药治疗相关的临床和经济结局。
从美国退伍军人健康管理局数据库中确定了 2013 年 10 月 1 日至 2018 年 3 月 31 日期间至少接受一种一线治疗(1L)的新诊断为 mRCC 的患者(索引日期=1L 开始日期)。评估了接受酪氨酸激酶抑制剂(TKI)、哺乳动物雷帕霉素靶蛋白抑制剂(mTOR)、免疫检查点抑制剂(ICI)和其他单药治疗的患者的治疗模式、临床结局(由非指数治疗的转换或指数治疗在 90 天以上的间隔后重新开始的最早时间定义的下一次治疗时间[TNT]、治疗终止时间[TTD]、总生存期[OS])和成本。采用标准描述性统计方法。采用 Kaplan-Meier 法评估临床结局。
在 759 名患者中(中位年龄 68.0 岁),分别有 85.0%、8.0%、4.3%和 2.6%接受了 TKI、mTOR、ICI 和其他单药治疗。进展率(进入二线[2L]治疗)范围为 10.0(ICI)至每 100 人年 45.1(TKI)。12 个月的 OS 率范围为 47.4%(TKI)至 67.7%(mTOR)。中位 TNT 范围为 3.8(mTOR)至 9.6 个月(ICI),中位 TTD 范围为 2.3(mTOR)至 4.7 个月(TKI)。每位患者每月的总全因平均费用范围为 12466 美元(mTOR)至 19812 美元(ICI)。
这些结果表明,接受一线单药治疗的 mRCC 患者存在高度未满足的医疗需求。新型联合疗法(例如,ICI+ICI、ICI+TKI)可能会改善预后不良患者的一线治疗结局。