Miao Yandong, Zhang Hongling, Su Bin, Wang Jiangtao, Quan Wuxia, Li Qiutian, Mi Denghai
The First Clinical Medical College, Lanzhou University, Lanzhou, Gansu, China.
Cancer Ward, Palliative Medical Center, New Kunhua Hospital, Kunming, Yunnan, China.
PeerJ. 2021 Apr 5;9:e11219. doi: 10.7717/peerj.11219. eCollection 2021.
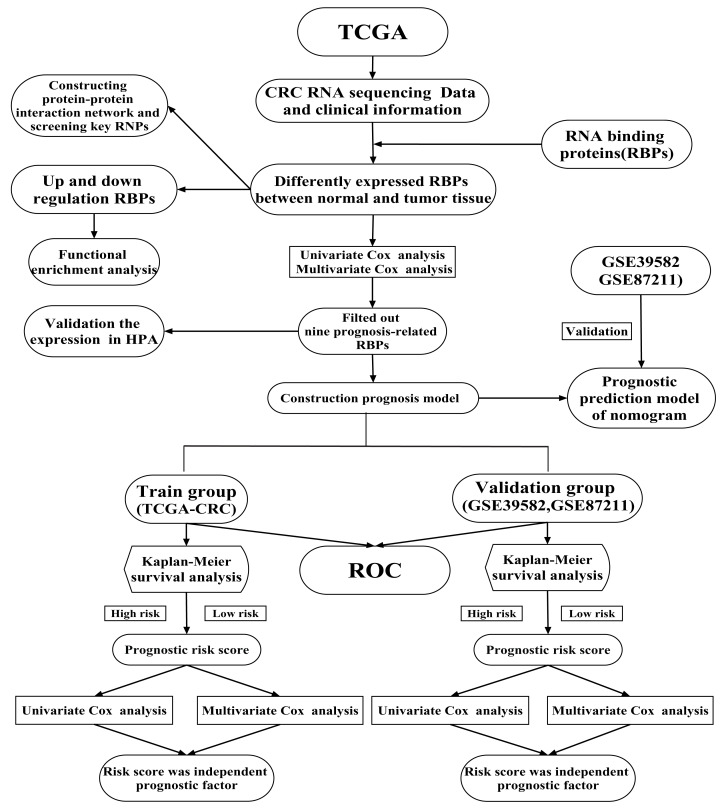
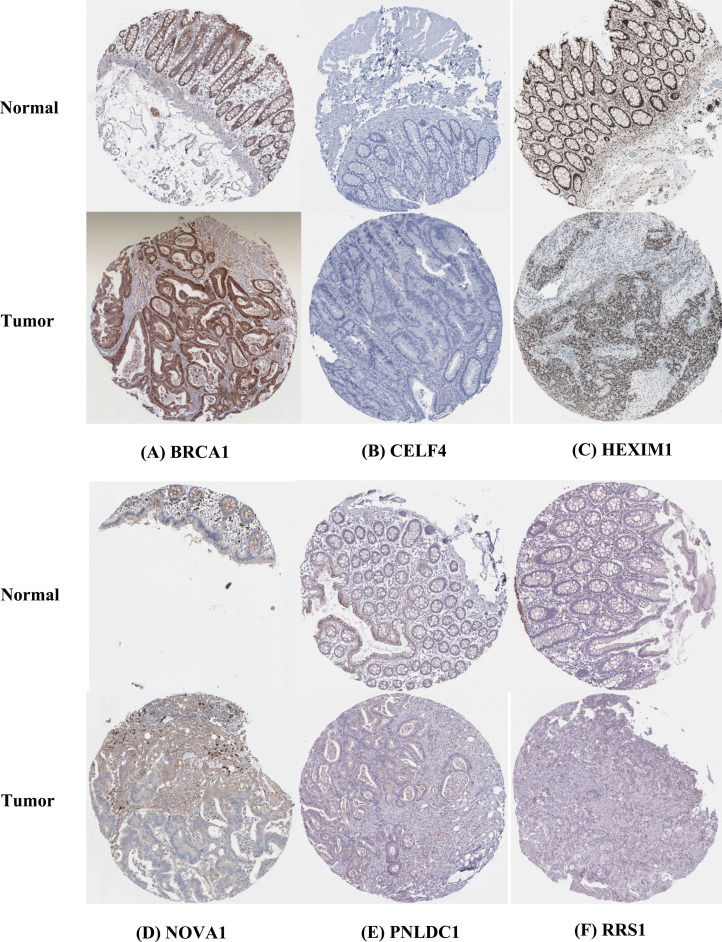
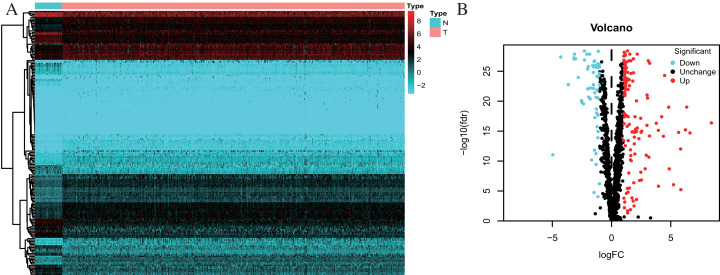
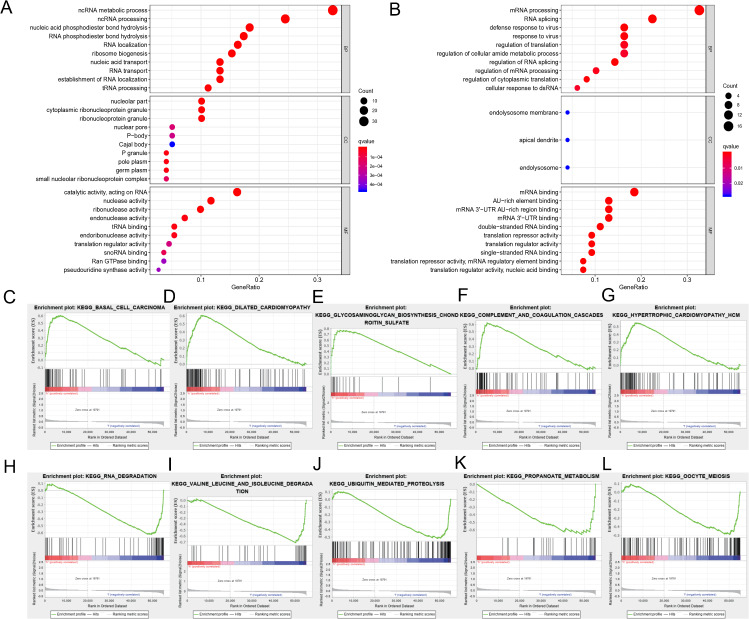
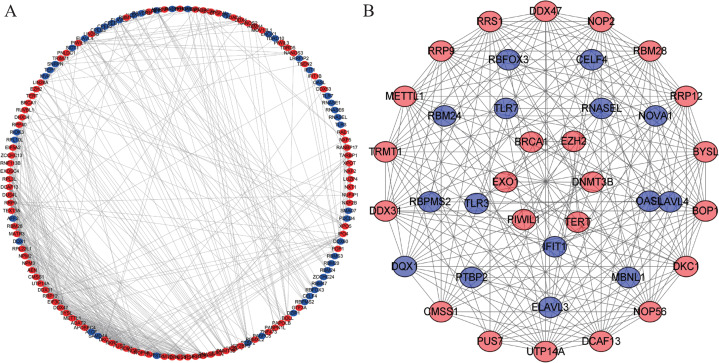
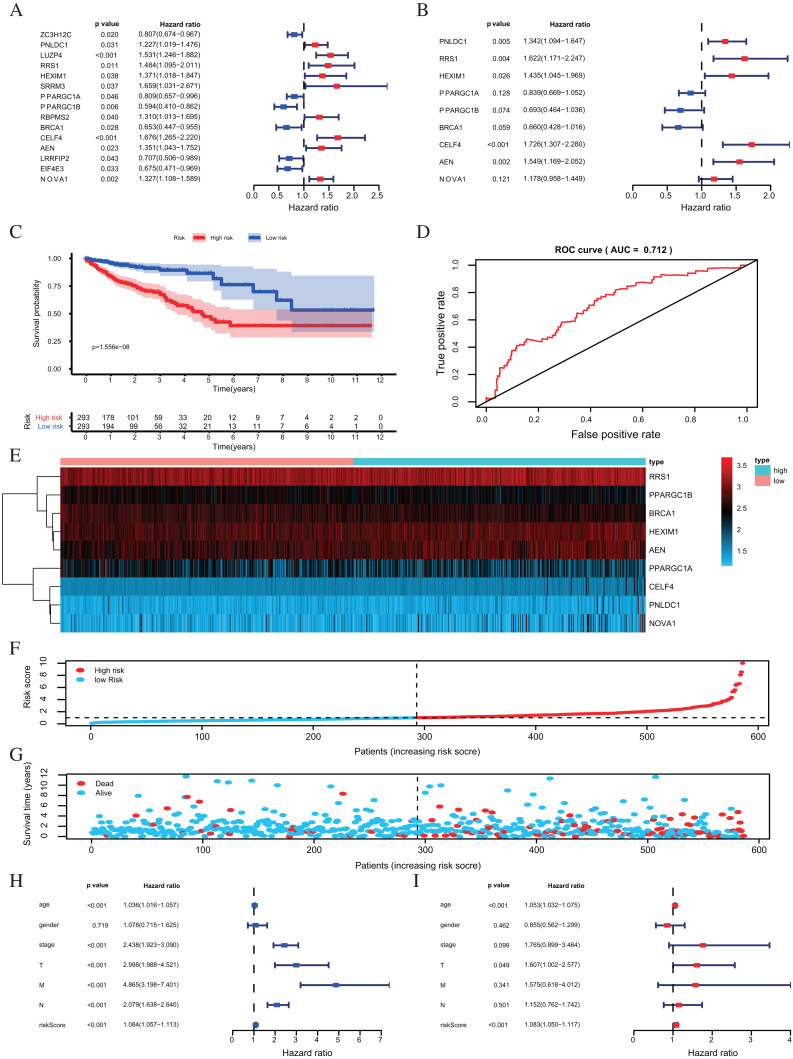
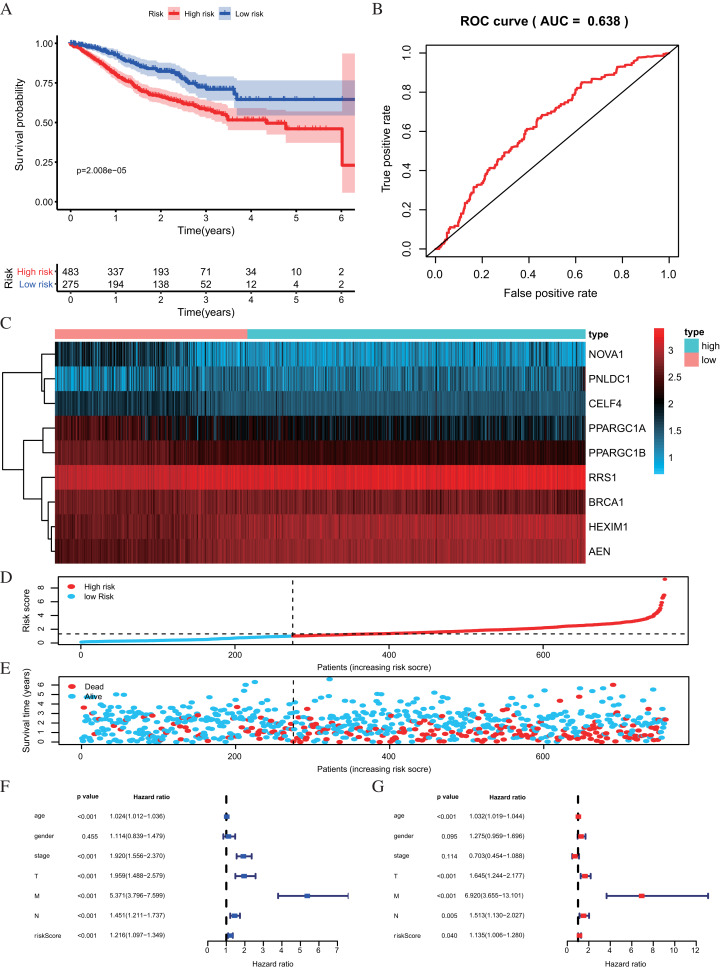
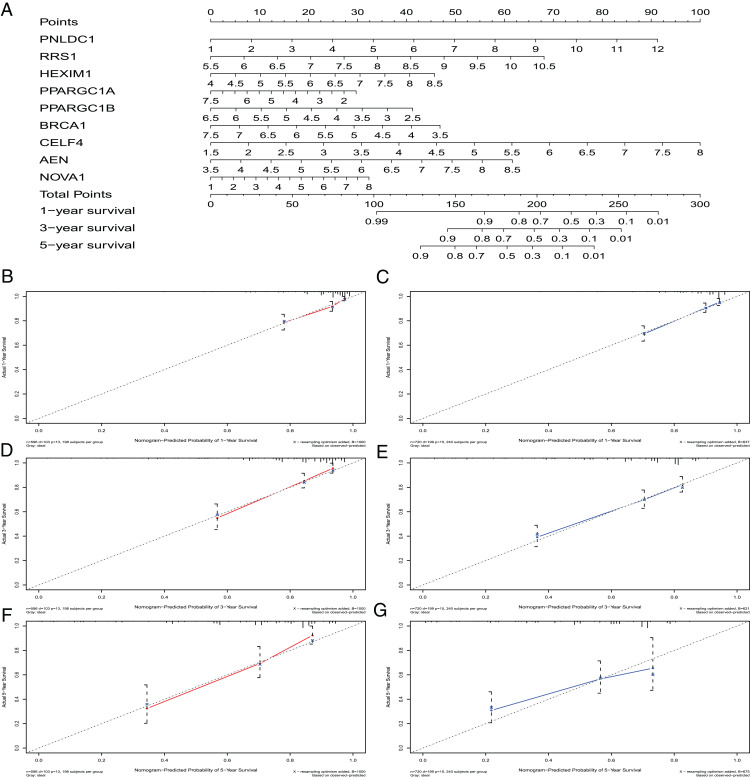
Colorectal cancer (CRC) is one of the most prevalent and fatal malignancies, and novel biomarkers for the diagnosis and prognosis of CRC must be identified. RNA-binding proteins (RBPs) are essential modulators of transcription and translation. They are frequently dysregulated in various cancers and are related to tumorigenesis and development. The mechanisms by which RBPs regulate CRC progression are poorly understood and no clinical prognostic model using RBPs has been reported in CRC. We sought to identify the hub prognosis-related RBPs and to construct a prognostic model for clinical use. mRNA sequencing and clinical data for CRC were obtained from The Cancer Genome Atlas database (TCGA). Gene expression profiles were analyzed to identify differentially expressed RBPs using R and Perl software. Hub RBPs were filtered out using univariate Cox and multivariate Cox regression analysis. We used functional enrichment analysis, including Gene Ontology and Gene Set Enrichment Analysis, to perform the function and mechanisms of the identified RBPs. The nomogram predicted overall survival (OS). Calibration curves were used to evaluate the consistency between the predicted and actual survival rate, the consistency index (c-index) was calculated, and the prognostic effect of the model was evaluated. Finally, we identified 178 differently expressed RBPs, including 121 up-regulated and 57 down-regulated proteins. Our prognostic model was based on nine RBPs (PNLDC1, RRS1, HEXIM1, PPARGC1A, PPARGC1B, BRCA1, CELF4, AEN and NOVA1). Survival analysis showed that patients in the high-risk subgroup had a worse OS than those in the low-risk subgroup. The area under the curve value of the receiver operating characteristic curve of the prognostic model is 0.712 in the TCGA cohort and 0.638 in the GEO cohort. These results show that the model has a moderate diagnostic ability. The c-index of the nomogram is 0.77 in the TCGA cohort and 0.73 in the GEO cohort. We showed that the risk score is an independent prognostic biomarker and that some RBPs may be potential biomarkers for the diagnosis and prognosis of CRC.
结直肠癌(CRC)是最常见且致命的恶性肿瘤之一,因此必须鉴定出用于CRC诊断和预后评估的新型生物标志物。RNA结合蛋白(RBPs)是转录和翻译的重要调节因子。它们在各种癌症中经常发生失调,并与肿瘤发生和发展相关。目前对RBPs调节CRC进展的机制了解甚少,且尚未有关于CRC中使用RBPs的临床预后模型的报道。我们试图鉴定出与预后相关的关键RBPs,并构建一个可供临床使用的预后模型。从癌症基因组图谱数据库(TCGA)获取CRC的mRNA测序数据和临床数据。使用R和Perl软件分析基因表达谱,以鉴定差异表达的RBPs。通过单变量Cox和多变量Cox回归分析筛选出关键RBPs。我们使用功能富集分析,包括基因本体论和基因集富集分析,来研究已鉴定RBPs的功能和机制。列线图预测总生存期(OS)。使用校准曲线评估预测生存率与实际生存率之间 的一致性,并计算一致性指数(c-index),从而评估模型的预后效果。最后,我们鉴定出178种差异表达的RBPs,其中包括121种上调蛋白和57种下调蛋白。我们的预后模型基于9种RBPs(PNLDC1、RRS1、HEXIM1、PPARGC1A、PPARGC1B、BRCA1、CELF4、AEN和NOVA1)。生存分析表明,高危亚组患者的OS比低危亚组患者更差。在TCGA队列中,预后模型的受试者工作特征曲线下面积值为0.712,在GEO队列中为0.638。这些结果表明该模型具有中等诊断能力。在TCGA队列中列线图的c-index为0.77,在GEO队列中为0.73。我们表明风险评分是一种独立的预后生物标志物,并且一些RBPs可能是CRC诊断和预后的潜在生物标志物。