Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, University of Washington, 325 9th Avenue, Seattle, WA, 98104, USA.
Sepsis Center of Research Excellence - University of Washington (SCORE-UW), Seattle, WA, USA.
Crit Care. 2021 Apr 19;25(1):148. doi: 10.1186/s13054-021-03547-z.
Analyses of blood biomarkers involved in the host response to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) viral infection can reveal distinct biological pathways and inform development and testing of therapeutics for COVID-19. Our objective was to evaluate host endothelial, epithelial and inflammatory biomarkers in COVID-19.
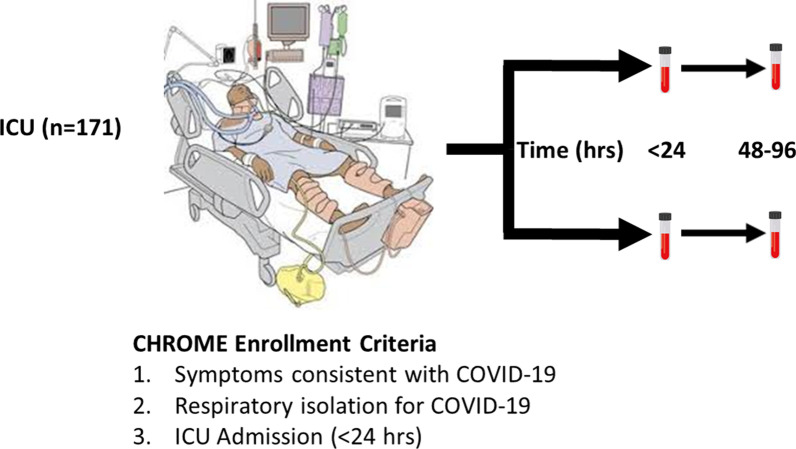
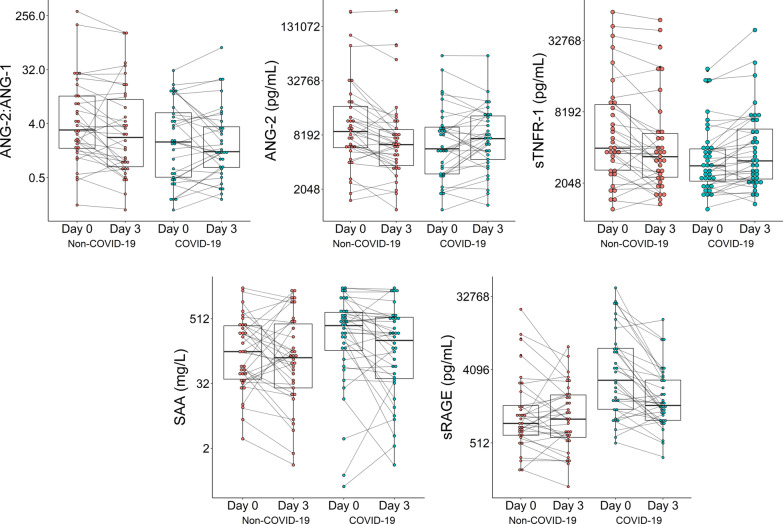
We prospectively enrolled 171 ICU patients, including 78 (46%) patients positive and 93 (54%) negative for SARS-CoV-2 infection from April to September, 2020. We compared 22 plasma biomarkers in blood collected within 24 h and 3 days after ICU admission.
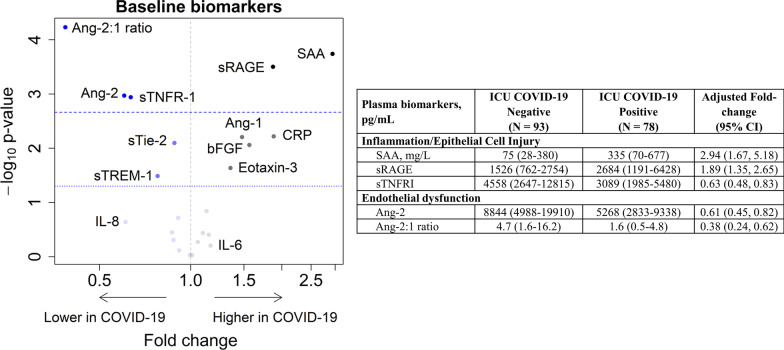
In critically ill COVID-19 and non-COVID-19 patients, the most common ICU admission diagnoses were respiratory failure or pneumonia, followed by sepsis and other diagnoses. Similar proportions of patients in both groups received invasive mechanical ventilation at the time of study enrollment. COVID-19 and non-COVID-19 patients had similar rates of acute respiratory distress syndrome, severe acute kidney injury, and in-hospital mortality. While concentrations of interleukin 6 and 8 were not different between groups, markers of epithelial cell injury (soluble receptor for advanced glycation end products, sRAGE) and acute phase proteins (serum amyloid A, SAA) were significantly higher in COVID-19 compared to non-COVID-19, adjusting for demographics and APACHE III scores. In contrast, angiopoietin 2:1 (Ang-2:1 ratio) and soluble tumor necrosis factor receptor 1 (sTNFR-1), markers of endothelial dysfunction and inflammation, were significantly lower in COVID-19 (p < 0.002). Ang-2:1 ratio and SAA were associated with mortality only in non-COVID-19 patients.
These studies demonstrate that, unlike other well-studied causes of critical illness, endothelial dysfunction may not be characteristic of severe COVID-19 early after ICU admission. Pathways resulting in elaboration of acute phase proteins and inducing epithelial cell injury may be promising targets for therapeutics in COVID-19.
分析宿主对严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)病毒感染的反应涉及的血液生物标志物,可以揭示不同的生物学途径,并为 COVID-19 的治疗药物的开发和测试提供信息。我们的目的是评估 COVID-19 中的宿主内皮细胞、上皮细胞和炎症生物标志物。
我们前瞻性地招募了 171 名 ICU 患者,其中 78 名(46%)患者 SARS-CoV-2 感染阳性,93 名(54%)患者 SARS-CoV-2 感染阴性,这些患者于 2020 年 4 月至 9 月期间入院。我们比较了 22 种在 ICU 入院后 24 小时和 3 天内采集的血液中的生物标志物。
在危重症 COVID-19 和非 COVID-19 患者中,最常见的 ICU 入院诊断是呼吸衰竭或肺炎,其次是脓毒症和其他诊断。在研究入组时,两组患者接受有创机械通气的比例相似。COVID-19 和非 COVID-19 患者的急性呼吸窘迫综合征、严重急性肾损伤和院内死亡率相似。虽然两组之间白细胞介素 6 和 8 的浓度没有差异,但上皮细胞损伤标志物(可溶性晚期糖基化终产物受体,sRAGE)和急性期蛋白(血清淀粉样蛋白 A,SAA)在 COVID-19 中明显高于非 COVID-19,调整了人口统计学和急性生理学和慢性健康评估 III 评分。相比之下,血管生成素 2:1(Ang-2:1 比值)和可溶性肿瘤坏死因子受体 1(sTNFR-1),内皮功能障碍和炎症的标志物,在 COVID-19 中明显较低(p < 0.002)。Ang-2:1 比值和 SAA 仅与非 COVID-19 患者的死亡率相关。
这些研究表明,与其他研究充分的危重病病因不同,内皮功能障碍可能不是 ICU 入院后早期严重 COVID-19 的特征。导致急性期蛋白产生和诱导上皮细胞损伤的途径可能是 COVID-19 治疗的有希望的靶点。