Yale School of Medicine, New Haven, Connecticut.
Department of Environmental Health Sciences, Yale School of Public Health, New Haven, Connecticut.
JAMA Netw Open. 2021 Apr 1;4(4):e217063. doi: 10.1001/jamanetworkopen.2021.7063.
Adequate representation of demographic subgroups in premarketing and postmarketing clinical studies is necessary for understanding the safety and efficacy associated with novel cancer therapeutics.
To characterize and compare the reporting of demographic data and the representation of individuals by sex, age, and race in premarketing and postmarketing studies used by the Food and Drug Administration (FDA) to evaluate novel cancer therapeutics.
DESIGN, SETTING, AND PARTICIPANTS: In this cross-sectional study, premarketing and postmarketing studies for novel cancer therapeutics approved by the FDA from 2012 through 2016 were identified. Study demographic information was abstracted from publicly available sources, and US cancer population demographic data was abstracted from US Cancer Statistics. Analyses were conducted from February 25 through September 21, 2020.
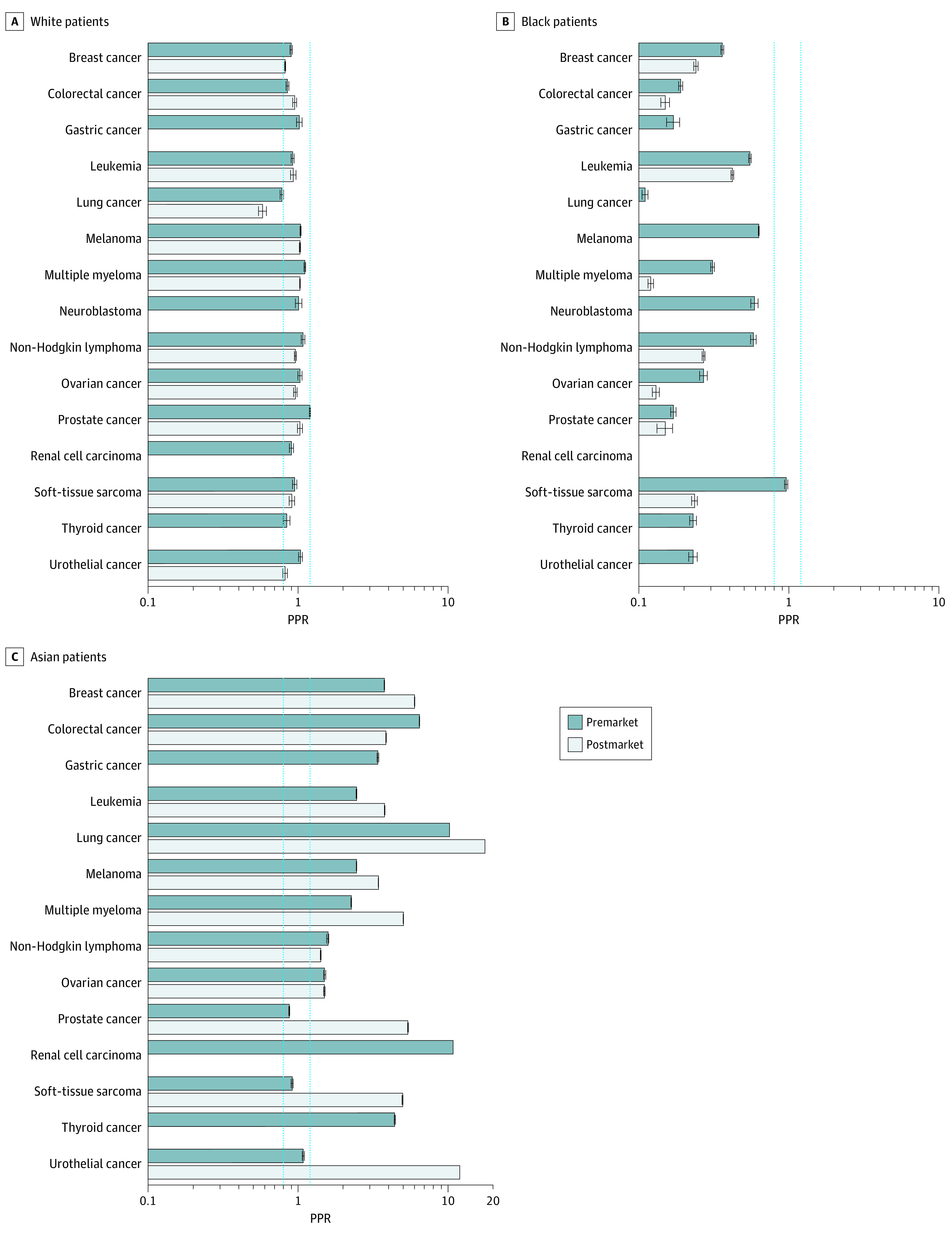
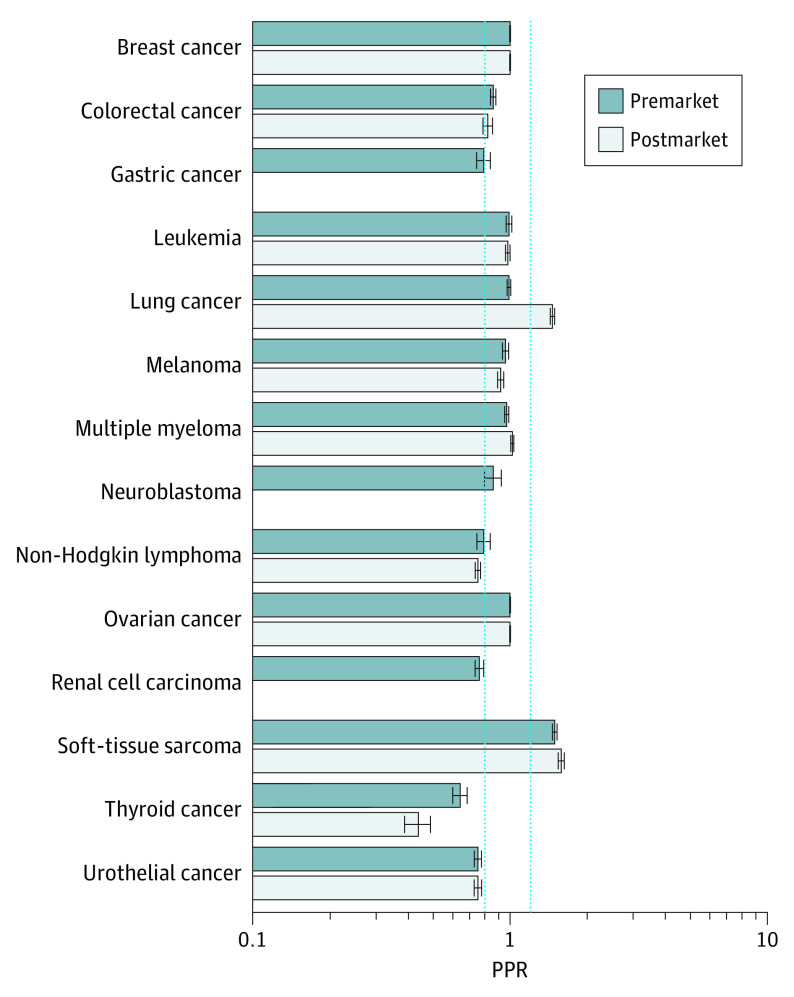
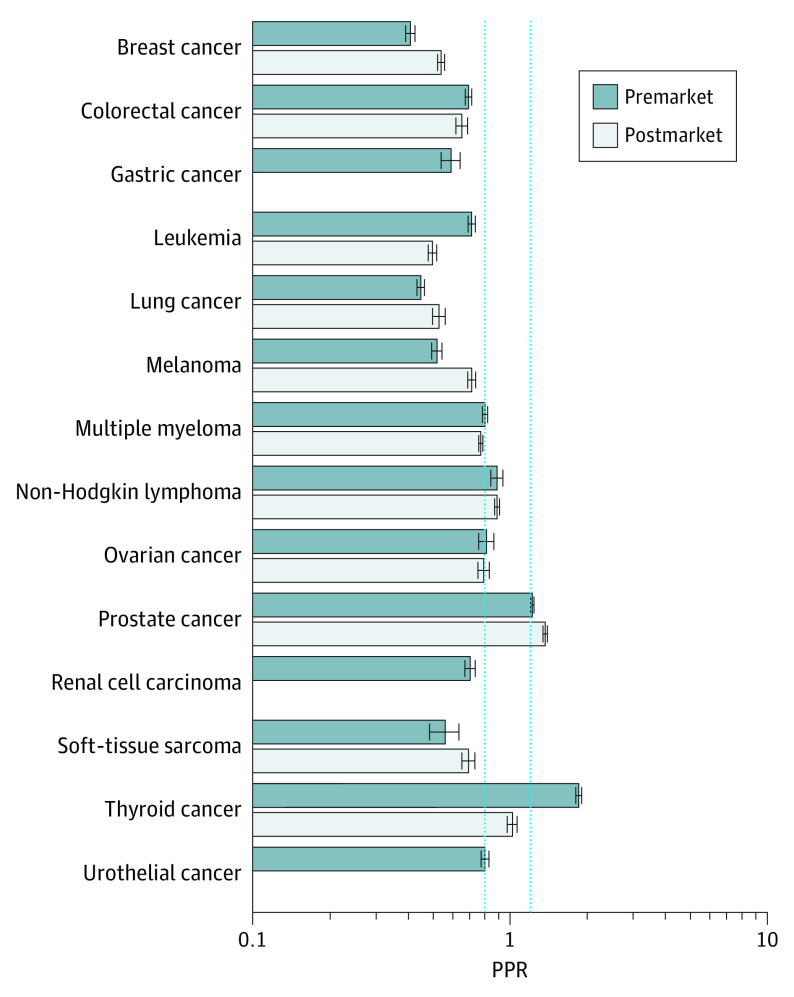
The percentages of trials reporting sex, age, and race/ethnicity were calculated, and participation to prevalence ratios (PPRs) were calculated by dividing the percentage of study participants in each demographic group by the percentage of the US cancer population in each group. PPRs were constructed for premarketing and postmarketing studies and by cancer type. Underrepresentation was defined as PPR less than 0.8.
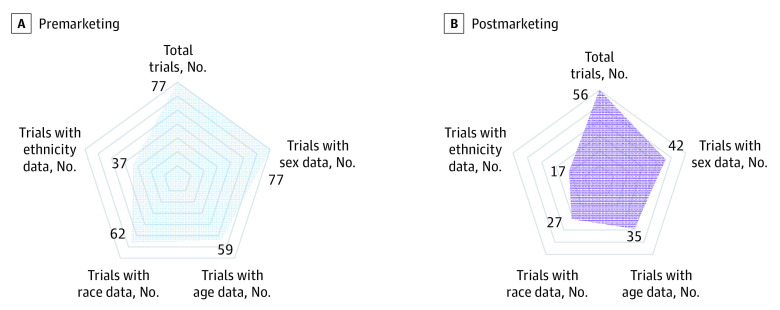
From 2012 through 2016, the FDA approved 45 cancer therapeutics. The study sample included 77 premarketing studies and 56 postmarketing studies. Postmarketing studies, compared with premarketing studies, were less likely to report patient sex (42 studies reporting [75.0%] vs 77 studies reporting [100%]; P < .001) and race (27 studies reporting [48.2%] vs 62 studies reporting [80.5%]; P < .001). Women were adequately represented in premarketing studies (mean [SD] PPR, 0.91; 95% CI, 0.90-0.91) and postmarketing studies (mean PPR, 1.00; 95% CI, 1.00-1.01). Although older adults and Black patients were underrepresented in premarketing studies (older adults: mean PPR, 0.73; 95% CI, 0.72-0.74; Black patients: mean PPR, 0.32; 95% CI, 0.31-0.32), these groups continued to be underrepresented in postmarketing studies (older adults: mean PPR, 0.75; 95% CI, 0.75-0.76; Black patients: mean PPR, 0.21; 95% CI, 0.21-0.21).
This study found that older adults and Black patients were underrepresented in postmarketing studies of novel cancer therapeutics to a similar degree that they were underrepresented in premarketing studies. These findings suggest that postmarketing studies are not associated with improvements to gaps in demographic representation present at the time of FDA approval.
在新药的临床前和临床研究中充分代表人口统计学亚组对于了解与新型癌症治疗相关的安全性和疗效是必要的。
描述和比较在 FDA 用于评估新型癌症治疗药物的临床前和临床研究中报告人口统计学数据和按性别、年龄和种族划分的个体代表性的情况。
设计、地点和参与者:在这项横断面研究中,确定了 2012 年至 2016 年期间 FDA 批准的新型癌症治疗药物的临床前和临床研究。从公开来源提取研究人口统计学信息,并从美国癌症统计数据中提取美国癌症人群的人口统计学数据。分析于 2020 年 2 月 25 日至 9 月 21 日进行。
计算了报告性别、年龄和种族/民族的试验百分比,并通过将每个人口统计学组的研究参与者百分比除以每个组的美国癌症人群百分比来计算参与率比值(PPR)。根据癌症类型,构建了临床前和临床研究的 PPR。代表性不足定义为 PPR 小于 0.8。
2012 年至 2016 年间,FDA 批准了 45 种癌症治疗药物。研究样本包括 77 项临床前研究和 56 项临床研究。与临床前研究相比,临床研究较少报告患者性别(42 项报告[75.0%] vs 77 项报告[100%];P<0.001)和种族(27 项报告[48.2%] vs 62 项报告[80.5%];P<0.001)。女性在临床前研究(平均[SD]PPR,0.91;95%CI,0.90-0.91)和临床研究(平均 PPR,1.00;95%CI,1.00-1.01)中得到充分代表。尽管老年人和黑人患者在临床前研究中代表性不足(老年人:平均 PPR,0.73;95%CI,0.72-0.74;黑人患者:平均 PPR,0.32;95%CI,0.31-0.32),但这些群体在临床研究中继续代表性不足(老年人:平均 PPR,0.75;95%CI,0.75-0.76;黑人患者:平均 PPR,0.21;95%CI,0.21-0.21)。
本研究发现,老年人和黑人患者在新型癌症治疗药物的临床研究中代表性不足的程度与临床前研究中代表性不足的程度相似。这些发现表明,临床研究与 FDA 批准时存在的人口统计学代表性差距的改善无关。