Rose Christian, Nichols Taylor, Hackner Daniel, Chang Julia, Straube Steven, Jooste Willem, Sawe Hendry, Tenner Andrea
Department of Emergency Medicine, Stanford University School of Medicine, Palo Alto, CA, United States.
Department of Emergency Medicine, University of California, San Francisco, San Francisco, CA, United States.
JMIR Form Res. 2021 May 26;5(5):e14851. doi: 10.2196/14851.
Health systems in low- and middle-income countries face considerable challenges in providing high-quality accessible care. eHealth has had mounting interest as a possible solution given the unprecedented growth in mobile phone and internet technologies in these locations; however, few apps or software programs have, as of yet, gone beyond the testing phase, most downloads are never opened, and consistent use is extremely rare. This is believed to be due to a failure to engage and meet local stakeholder needs and the high costs of software development.
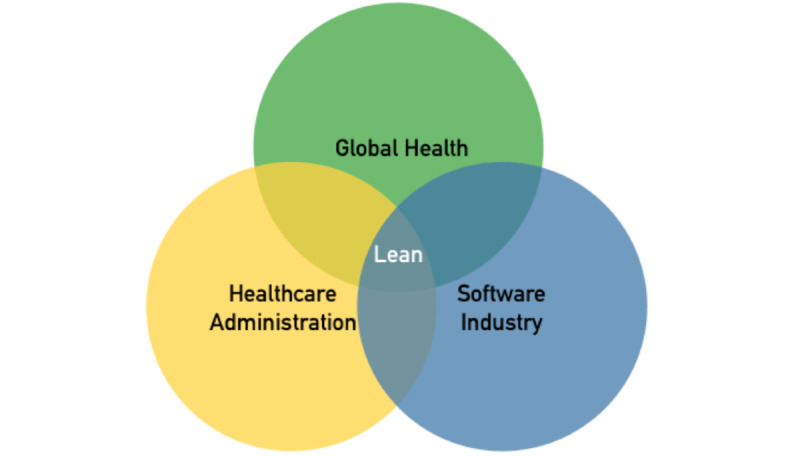
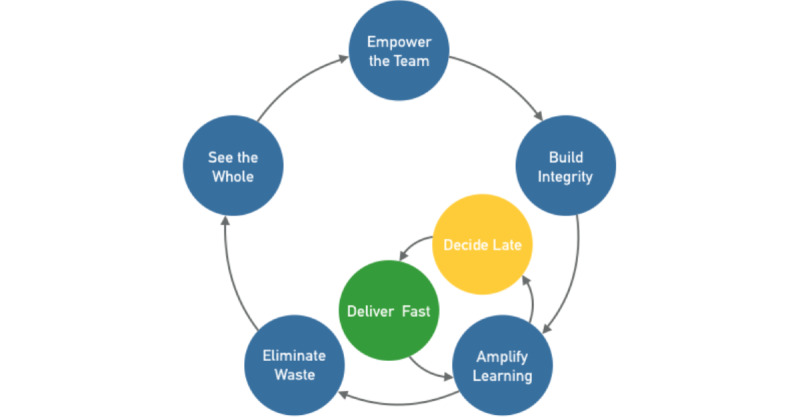
World Health Organization Basic Emergency Care course participants requested a mobile point-of-care adjunct to the primary course material. Our team undertook the task of developing this solution through a community-based participatory model in an effort to meet trainees' reported needs and avoid some of the abovementioned failings. We aimed to use the well-described Lean software development strategy-given our familiarity with its elements and its ubiquitous use in medicine, global health, and software development-to complete this task efficiently and with maximal stakeholder involvement.
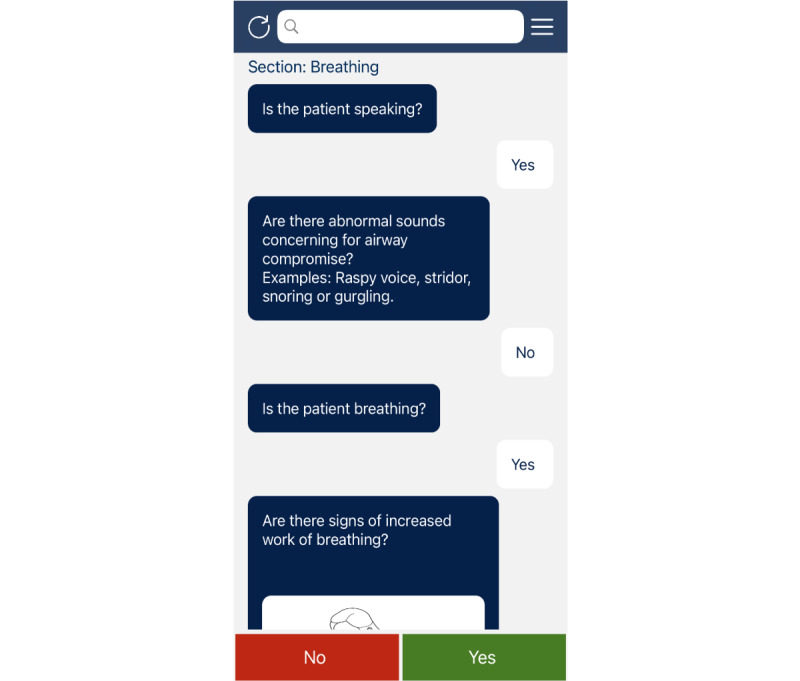
From September 2016 through January 2017, the Basic Emergency Care app was designed and developed at the University of California San Francisco. When a prototype was complete, it was piloted in Cape Town, South Africa and Dar es Salaam, Tanzania-World Health Organization Basic Emergency Care partner sites. Feedback from this pilot shaped continuous amendments to the app before subsequent user testing and study of the effect of use of the app on trainee retention of Basic Emergency Care course material.
Our user-centered mobile app was developed with an iterative participatory approach with its first version available within 6 months and with high acceptance-95% of Basic Emergency Care Course participants felt that it was useful. Our solution had minimal direct costs and resulted in a robust infrastructure for subsequent assessment and maintenance and allows for efficient feedback and expansion.
We believe that utilizing Lean software development strategies may help global health advocates and researchers build eHealth solutions with a process that is familiar and with buy-in across stakeholders that is responsive, rapid to deploy, and sustainable.
低收入和中等收入国家的卫生系统在提供高质量的可及医疗服务方面面临巨大挑战。鉴于这些地区手机和互联网技术前所未有的增长,电子健康作为一种可能的解决方案受到越来越多的关注;然而,截至目前,很少有应用程序或软件程序超出测试阶段,大多数下载后从未打开,持续使用极为罕见。据信,这是由于未能吸引并满足当地利益相关者的需求以及软件开发成本高昂。
世界卫生组织基础急救课程的参与者要求为初级课程材料配备一个移动医疗点辅助工具。我们的团队通过基于社区的参与式模型承担了开发此解决方案的任务,以满足学员报告的需求并避免上述一些不足。鉴于我们熟悉精益软件开发策略的要素及其在医学、全球卫生和软件开发中的广泛应用,我们旨在利用该策略高效地完成这项任务,并让利益相关者最大限度地参与进来。
2016年9月至2017年1月,基础急救应用程序在加利福尼亚大学旧金山分校进行设计和开发。当原型完成后,在南非开普敦和坦桑尼亚达累斯萨拉姆——世界卫生组织基础急救合作伙伴站点进行了试点。此次试点的反馈为应用程序的持续修改提供了依据,随后进行了用户测试以及对应用程序使用对学员掌握基础急救课程材料效果的研究。
我们以用户为中心的移动应用程序采用迭代式参与方法开发,其第一个版本在6个月内可用,并且接受度很高——95%的基础急救课程参与者认为它很有用。我们的解决方案直接成本最低,并为后续评估和维护建立了强大的基础设施,还能实现高效反馈和扩展。
我们认为,利用精益软件开发策略可能有助于全球卫生倡导者和研究人员构建电子健康解决方案,其过程为人所熟知,且能获得利益相关者的认可,具有响应迅速、部署快速和可持续的特点。