Division of General Internal Medicine, Department of Medicine, Albert Einstein College of Medicine & Montefiore Medical Center, Bronx, New York, USA.
Departments of Epidemiology & Global Health, Rollins School of Public Health, Emory University, Atlanta, Georgia, USA.
Clin Infect Dis. 2021 Dec 6;73(11):2083-2092. doi: 10.1093/cid/ciab335.
Bedaquiline improves treatment outcomes in patients with rifampin-resistant (RR) tuberculosis but prolongs the QT interval and carries a black-box warning from the US Food and Drug Administration. The World Health Organization recommends that all patients with RR tuberculosis receive a regimen containing bedaquiline, yet a phase 3 clinical trial demonstrating its cardiac safety has not been published.
We conducted an observational cohort study of patients with RR tuberculosis from 3 provinces in South Africa who received regimens containing bedaquiline. We performed rigorous cardiac monitoring, which included obtaining electrocardiograms in triplicate at 4 time points during bedaquiline therapy. Participants were followed up until the end of therapy or 24 months. Outcomes included final tuberculosis treatment outcome and QT interval prolongation (QT prolongation), defined as any QT interval corrected by the Fridericia method (QTcF) >500 ms or an absolute change from baseline (ΔQTcF) >60 ms.
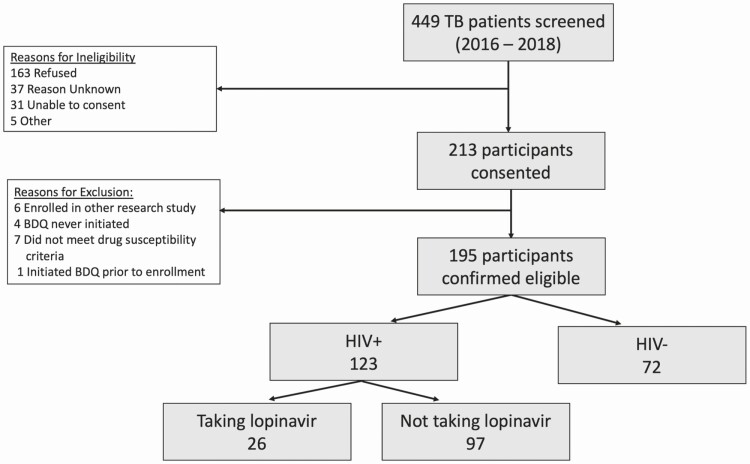
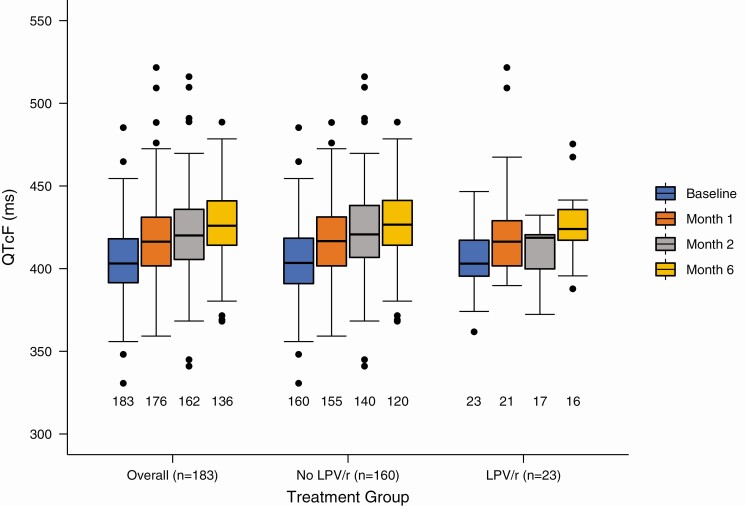
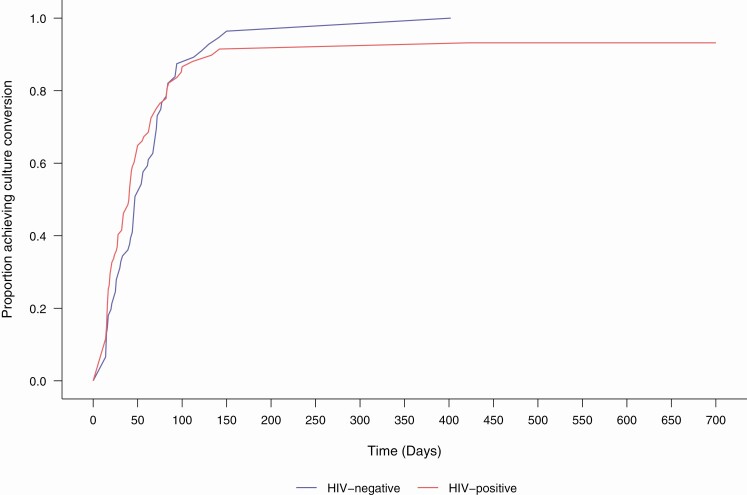
We enrolled 195 eligible participants, of whom 40% had extensively drug-resistant tuberculosis. Most participants (97%) received concurrent clofazimine. Of the participants, 74% were cured or successfully completed treatment, and outcomes did not differ by human immunodeficiency virus status. QTcF continued to increase throughout bedaquiline therapy, with a mean increase (standard deviation) of 23.7 (22.7) ms from baseline to month 6. Four participants experienced a QTcF >500 ms and 19 experienced a ΔQTcF >60 ms. Older age was independently associated with QT prolongation. QT prolongation was neither more common nor more severe in participants receiving concurrent lopinavir-ritonavir.
Severe QT prolongation was uncommon and did not require permanent discontinuation of either bedaquiline or clofazimine. Close monitoring of the QT interval may be advisable in older patients.
贝达喹啉可改善耐利福平(RR)结核病患者的治疗效果,但会延长 QT 间期,并收到美国食品和药物管理局的黑框警告。世界卫生组织建议所有 RR 结核病患者接受包含贝达喹啉的方案治疗,但尚未公布证明其心脏安全性的 III 期临床试验。
我们对南非 3 个省份接受包含贝达喹啉方案治疗的 RR 结核病患者进行了一项观察性队列研究。我们进行了严格的心脏监测,包括在贝达喹啉治疗的 4 个时间点重复进行 3 次心电图检查。参与者随访至治疗结束或 24 个月。结局包括最终结核病治疗结局和 QT 间期延长(QT 延长),定义为任何 Fridericia 法校正 QT 间期(QTcF)>500 ms 或与基线相比的绝对变化(ΔQTcF)>60 ms。
我们纳入了 195 名符合条件的参与者,其中 40%患有广泛耐药结核病。大多数参与者(97%)同时接受氯法齐明治疗。其中 74%的参与者治愈或成功完成治疗,结局与人类免疫缺陷病毒状态无关。在整个贝达喹啉治疗期间,QTcF 持续增加,从基线到第 6 个月的平均增加(标准差)为 23.7(22.7)ms。4 名参与者出现 QTcF>500 ms,19 名参与者出现 ΔQTcF>60 ms。年龄较大与 QT 延长独立相关。同时接受洛匹那韦/利托那韦治疗的参与者中,QT 延长既不更常见也不更严重。
严重的 QT 延长并不常见,且不需要永久停用贝达喹啉或氯法齐明。在老年患者中可能需要密切监测 QT 间期。