Department of Medical Microbiology, University of Zimbabwe College of Health Sciences, Harare, Zimbabwe.
Infections and Cancer Biology Group, International Agency for Research on Cancer, Lyon, France.
PLoS One. 2021 Apr 26;16(4):e0250426. doi: 10.1371/journal.pone.0250426. eCollection 2021.
BACKGROUND & AIM: Women with HIV/HPV coinfection and cervical lesions are at increased risk of developing HPV related anal cancer. Self-collection of anal swabs may facilitate HPV molecular testing in anal cancer screening, especially in high-risk groups, and yet it is not adequately studied. We evaluated level of agreement between self-collected anal swabs (SCAS) and clinician-collected anal swabs (CCAS) when used for HPV genotyping. We also described the anal HPV genotype distribution and HIV/HPV coinfection.
We performed a cross sectional study with participants from a visual-inspection-with-acetic-acid and cervicography (VIAC) clinic, in Harare, Zimbabwe. In a clinic setting, the women aged ≥18 years provided anal swabs in duplicate; first CCAS and then SCAS immediately after. HPV detection and genotyping were performed using next generation amplicon sequencing of a 450bp region of the HPV L1 gene. Level of agreement of HPV genotypes between CCAS and SCAS was calculated using the kappa statistic. McNemar tests were used to evaluate agreement in the proportion of genotypes detected by either method.
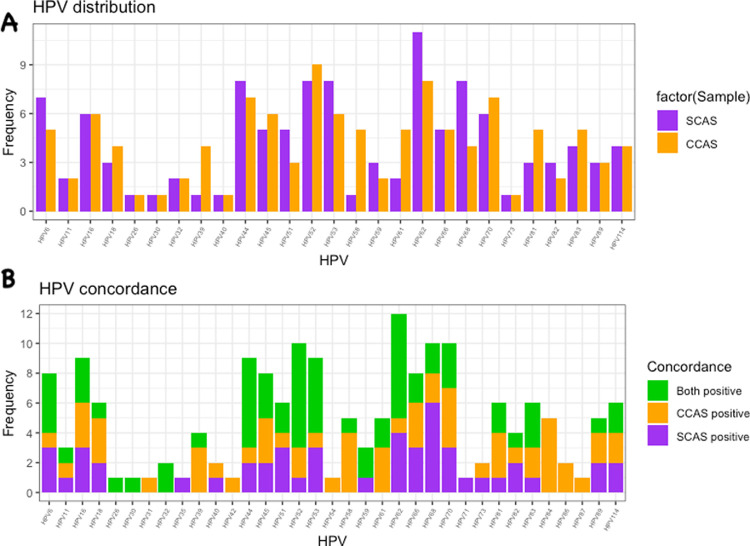
Three-hundred women provided 600 samples for HPV genotyping. HPV genotypes were detected in 25% of SCAS and in 22% of CCAS. The most common genotypes with CCAS were HPV52, HPV62 and HPV70 and with SCAS were HPV62, HPV44, HPV52, HPV53 and HPV68. Total HPV genotypes detected in CCAS were more than those detected in SCAS, 32 versus 27. The agreement of HPV genotypes between the two methods was 0.55 in kappa value (k). The test of proportions using McNemar gave a Chi-square value of 0.75 (p = 0.39). Multiple HPV infections were detected in 28/75 and 29/67 women for CCAS and SCAS respectively.
SCAS and CCAS anal swabs showed moderate agreement, with no statistically significant difference in the proportion of genotypes detected by either methods. Although the differences between the two methods were not statistically significant, CCAS detected more HPV genotypes than SCAS and more HPV infections were detected in SCAS than in CCAS. Our data suggest that self-collected anal swabs can be used as an alternative to clinician-collected anal swabs for HPV genotyping.
HIV/HPV 合并感染且存在宫颈病变的女性发生 HPV 相关肛门癌的风险增加。自我采集肛门拭子可能有助于肛门癌筛查中的 HPV 分子检测,尤其是在高危人群中,但目前对其研究尚不充分。我们评估了自我采集肛门拭子(SCAS)和临床医生采集肛门拭子(CCAS)在 HPV 基因分型中的一致性。我们还描述了肛门 HPV 基因型分布和 HIV/HPV 合并感染情况。
我们在津巴布韦哈拉雷的醋酸视觉检查和宫颈涂片(VIAC)诊所进行了一项横断面研究,纳入年龄≥18 岁的参与者。在诊所环境中,这些女性同时提供两份肛门拭子,先采集 CCAS,然后紧接着采集 SCAS。使用 HPV L1 基因 450bp 区域的下一代扩增子测序来检测和分型 HPV。使用 Kappa 统计量计算 CCAS 和 SCAS 之间 HPV 基因型的一致性。McNemar 检验用于评估两种方法检测到的基因型比例的一致性。
300 名女性共提供 600 份用于 HPV 基因分型的样本。25%的 SCAS 和 22%的 CCAS 检测到 HPV 基因型。CCAS 最常见的基因型为 HPV52、HPV62 和 HPV70,SCAS 最常见的基因型为 HPV62、HPV44、HPV52、HPV53 和 HPV68。CCAS 检测到的总 HPV 基因型多于 SCAS,分别为 32 种和 27 种。两种方法检测 HPV 基因型的一致性为 Kappa 值 0.55(k)。McNemar 检验的比例检验值为 0.75(p=0.39)。CCAS 和 SCAS 分别有 28/75 和 29/67 名女性检测到多重 HPV 感染。
SCAS 和 CCAS 肛门拭子显示出中等程度的一致性,两种方法检测到的基因型比例无统计学差异。尽管两种方法之间的差异无统计学意义,但 CCAS 检测到的 HPV 基因型多于 SCAS,SCAS 检测到的 HPV 感染多于 CCAS。我们的数据表明,自我采集的肛门拭子可替代临床医生采集的肛门拭子用于 HPV 基因分型。