Department of Emergency Medicine, Columbia University, 622 W. 168th Street, New York, NY 10032, United States.
Columbia University Vagelos College of Physicians & Surgeons, 630 W. 168th Street, New York, NY 10032, United States.
Am J Emerg Med. 2021 Sep;47:213-216. doi: 10.1016/j.ajem.2021.04.063. Epub 2021 Apr 23.
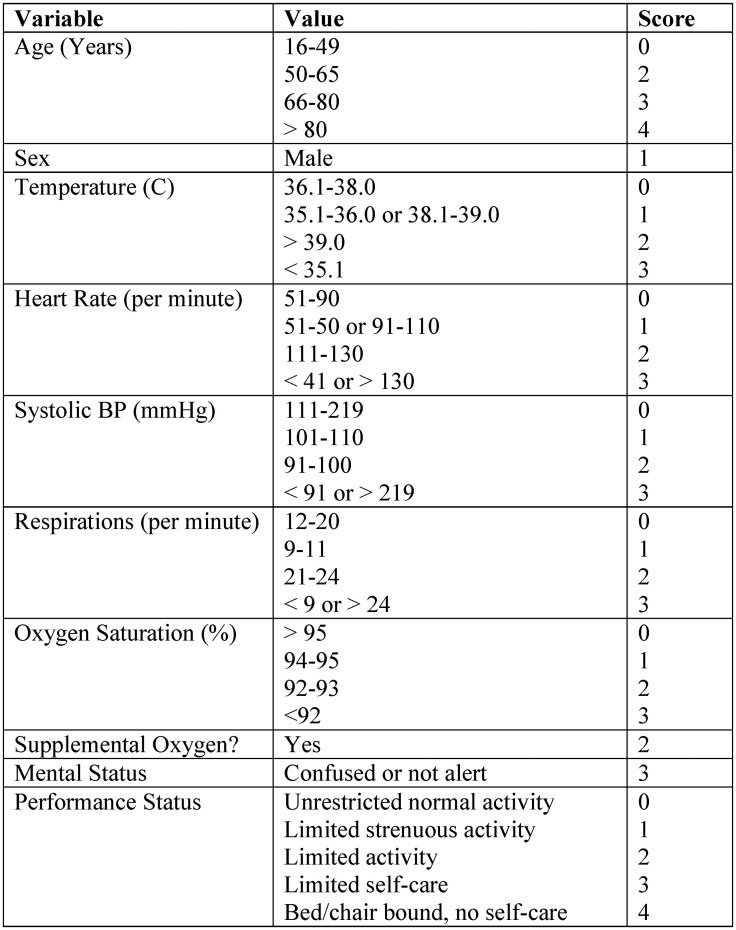
COVID-19 transmission remains high around the world, and severe local outbreaks continue to occur. Prognostic tools may be useful in crisis conditions as risk stratification can help determine resource allocation. One published tool, the Pandemic Respiratory Infection Emergency System Triage Severity Score, seems particularly promising because of its predictive ability and ease of application at the bedside. We sought to understand the performance of a modified version of this score (mPRIEST) in our institution for identifying patients with a greater than minimal risk for adverse outcome (death or organ support) at 30 days after index visit.
Consecutive visits at two northern Manhattan EDs with a new diagnosis of symptomatic COVID-19 were identified between November and December of 2020. Demographic variables and clinical characteristics were obtained from chart review. Outcomes were obtained from chart review and follow-up phone call.
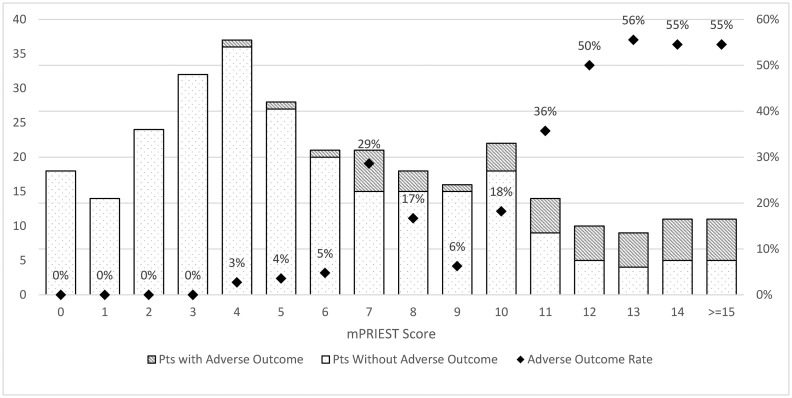
Outcomes were available on 306 patients. The incidence of death or mechanical ventilation at 30 days for patients in patients with mPRIEST above the threshold value was 43/181 (23.8%), and for patients below 1/125 (0.8%). The sensitivity of the score for adverse outcome was 97.7% (95% CI: 93.3% to 100%).
This data suggests the mPRIEST score, which can be calculated from clinical variables alone, has potential for use in EDs to identify patients at very low risk for adverse outcomes within 30 days of COVID diagnosis. This should be confirmed in larger formal validation studies in diverse settings.
COVID-19 在全球范围内的传播仍然很高,严重的局部爆发仍在继续发生。预测工具在危机情况下可能很有用,因为风险分层有助于确定资源分配。一种已发表的工具,即大流行呼吸道感染紧急系统分诊严重程度评分,由于其预测能力和在床边应用的简便性,似乎特别有希望。我们试图了解该评分的改良版本(mPRIEST)在我们机构中的表现,以确定在指数就诊后 30 天内有不良结局(死亡或器官支持)风险大于最小风险的患者。
在 2020 年 11 月至 12 月期间,确定了两个位于曼哈顿北部的急诊科连续出现新诊断为有症状 COVID-19 的就诊患者。从病历回顾中获得人口统计学变量和临床特征。从病历回顾和随访电话中获得结局。
在 306 名患者中获得了结局。mPRIEST 阈值以上的患者在 30 天内死亡或机械通气的发生率为 43/181(23.8%),而 mPRIEST 阈值以下的患者为 1/125(0.8%)。该评分对不良结局的敏感性为 97.7%(95%CI:93.3%至 100%)。
这些数据表明,mPRIEST 评分可以仅根据临床变量计算,具有在急诊科识别 COVID 诊断后 30 天内不良结局风险非常低的患者的潜力。这应在不同环境下的更大规模正式验证研究中得到证实。