Shi Zhang, Li Jing, Zhao Ming, Zhang Minmin, Wang Tiegong, Chen Luguang, Liu Qi, Wang He, Lu Jianping, Zhao Xihai
Department of Radiology, Changhai Hospital, Naval Medical University, Shanghai, China.
Department of Neurology, The 983th Hospital of Joint Logistics Support Forces of Chinese PLA, Tianjin, China.
Front Neurosci. 2021 Apr 12;15:608799. doi: 10.3389/fnins.2021.608799. eCollection 2021.
This study aims to investigate the agreement of three software packages in measuring baseline ischemic core volume (ICV) and penumbra volume (PV), and determine their predictive values for unfavorable clinical outcome in patients with endovascular thrombectomy (EVT).
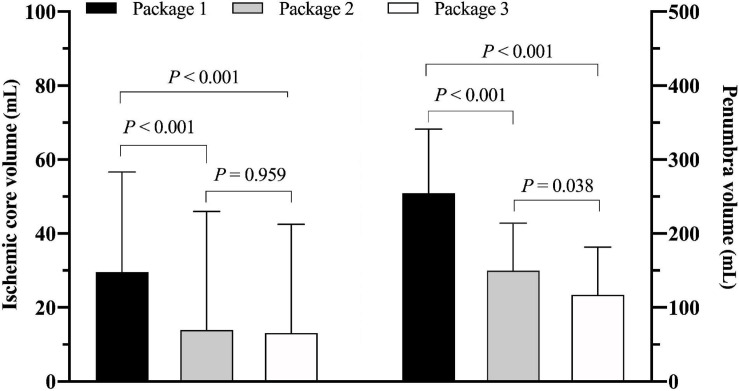
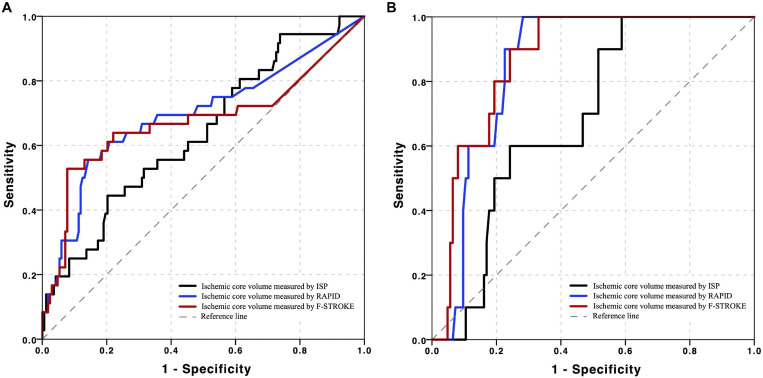
Patients with acute ischemic stroke who underwent computed tomographic perfusion (CTP) were recruited. Baseline CTP measurements including ICV and PV were calculated by three software packages of IntelliSpace Portal (ISP), Rapid Processing of Perfusion and Diffusion (RAPID), and fast-processing of ischemic stroke (F-STROKE). All patients received EVT, and the modified Rankin scale (mRS) at 90 days after EVT was assessed to determine the clinical outcomes (favorable: mRS = 0-2; unfavorable: mRS = 3-6). The agreement of CTP measurements among three software packages was determined using intraclass correlation coefficient (ICC). The associations between CTP measurements and unfavorable clinical outcome were analyzed using logistic regression. Receiver operating characteristic curves were conducted to calculate the area under the curve (AUC) of CTP measurements in predicting unfavorable clinical outcome.
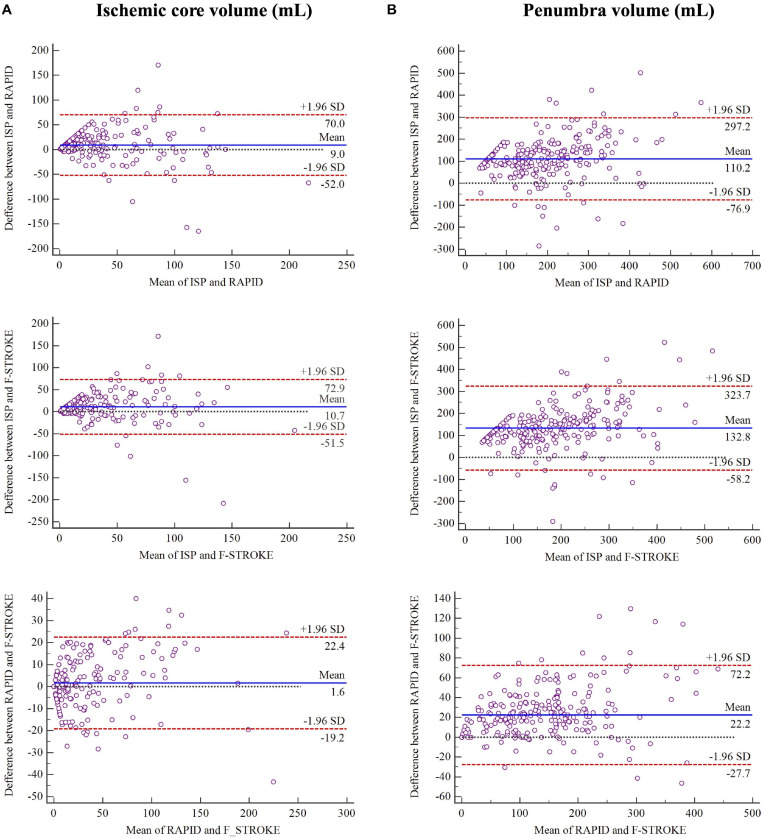
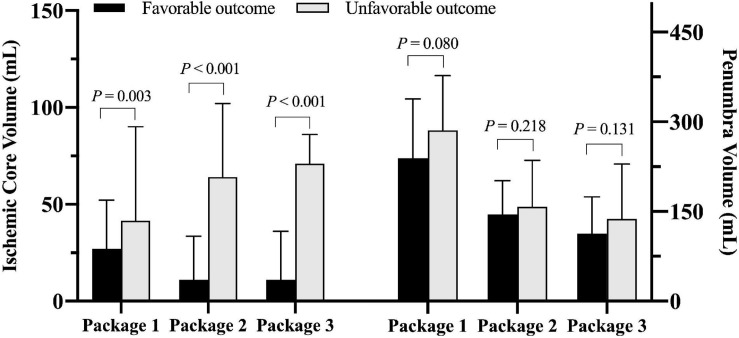
Of 223 recruited patients (68.2 ± 11.3 years old; 145 males), 17.0% had unfavorable clinical outcome after EVT. Excellent agreement between F-STROKE and RAPID was found in measuring ICV (ICC 0.965; 95% CI 0.956-0.973) and PV (ICC 0.966; 95% CI 0.956-0.973). ICVs measured by three software packages were significantly associated with unfavorable clinical outcome before (odds ratios 1.012-1.018, all < 0.01) and after (odds ratios 1.003-1.014, all < 0.05) adjusted for confounding factors (age, gender, TOAST classification, and NIHSS on admission). In predicting unfavorable clinical outcome, ICV measured by F-STROKE showed similar performance to that measured by RAPID (AUC 0.701 vs. 0.717) but higher performance than that measured by ISP (AUC 0.629).
The software of F-STROKE has excellent agreement with the widely used analysis tool of RAPID in measuring ICV and PV. The ischemic core volume measured by both F-STROKE and RAPID is a stronger predictor for unfavorable clinical outcome after EVT compared to ISP.
本研究旨在探讨三款软件包在测量基线缺血核心体积(ICV)和半暗带体积(PV)方面的一致性,并确定它们对血管内血栓切除术(EVT)患者不良临床结局的预测价值。
招募接受计算机断层扫描灌注(CTP)的急性缺血性卒中患者。通过IntelliSpace Portal(ISP)、灌注与扩散快速处理(RAPID)和缺血性卒中快速处理(F-STROKE)三款软件包计算包括ICV和PV在内的基线CTP测量值。所有患者均接受了EVT,并在EVT后90天评估改良Rankin量表(mRS)以确定临床结局(良好:mRS = 0-2;不良:mRS = 3-6)。使用组内相关系数(ICC)确定三款软件包之间CTP测量值的一致性。使用逻辑回归分析CTP测量值与不良临床结局之间的关联。绘制受试者工作特征曲线以计算CTP测量值在预测不良临床结局方面的曲线下面积(AUC)。
在招募的223例患者(68.2±11.3岁;145例男性)中,17.0%在EVT后出现不良临床结局。在测量ICV(ICC 0.965;95%CI 0.956-0.973)和PV(ICC 0.966;95%CI 0.956-0.973)方面,F-STROKE与RAPID之间具有极好的一致性。在调整混杂因素(年龄、性别、TOAST分类和入院时的美国国立卫生研究院卒中量表评分)之前(比值比1.012-1.018,均<0.01)和之后(比值比1.003-1.014,均<0.05),三款软件包测量的ICV均与不良临床结局显著相关。在预测不良临床结局方面,F-STROKE测量的ICV表现与RAPID测量的相似(AUC 0.701对0.717),但优于ISP测量的(AUC 0.629)。
F-STROKE软件在测量ICV和PV方面与广泛使用的分析工具RAPID具有极好的一致性。与ISP相比,F-STROKE和RAPID测量的缺血核心体积对EVT后不良临床结局的预测性更强。