Roccatello Dario, Sciascia Savino, Naretto Carla, Alpa Mirella, Fenoglio Roberta, Ferro Michela, Quattrocchio Giacomo, Rubini Elena, Rahbani Elnaz, Rossi Daniela
CMID-Nephrology and Dialysis Unit (ERK-net Member), Center of Research of Immunopathology and Rare Diseases, Coordinating Center of the Network for Rare Diseases of Piedmont and Aosta Valley, Department of Clinical and Biological Sciences, University of Turin and S. Giovanni Bosco Hub Hospital, Turin, Italy.
Kidney Int Rep. 2021 Feb 3;6(4):1081-1087. doi: 10.1016/j.ekir.2021.01.027. eCollection 2021 Apr.
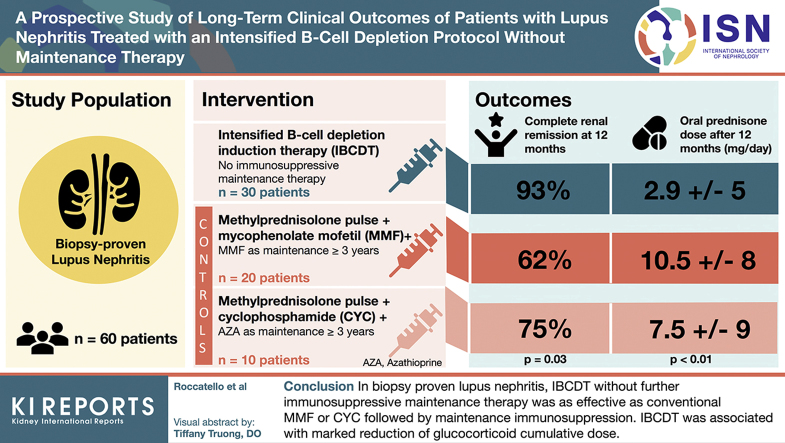
We aimed to investigate the safety and efficacy of an intensified B-cell depletion induction therapy (IBCDT) without immunosuppressive maintenance regimen compared with standard of care in biopsy-proven lupus nephritis (LN).
Thirty patients were administered an IBCDT (4 weekly rituximab [RTX] 375 mg/m and 2 more doses after 1 and 2 months; 2 infusions of 10 mg/kg cyclophosphamide [CYC], 3 methylprednisolone pulses), followed by oral prednisone (tapered to 5 mg/d by the third month). No immunosuppressive maintenance therapy was given. Thirty patients matched for LN class and age were selected as controls: 20 received 3 methylprednisolone pulses days followed by oral prednisone and mycophenolate mofetil (MMF) 2 to 3 g/d, whereas 10 were given the Euro Lupus CYC. MMF (1-2 g/daily) or azathioprine (AZA, 1-2 mg/kg/day) were given for > 3 years as a maintenance therapy.
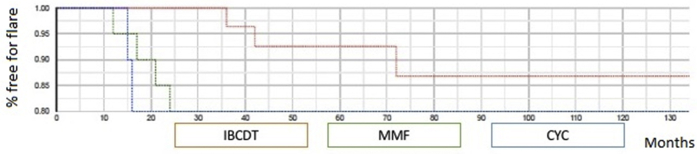
At 12 months, complete renal remission was observed in 93% of patients on IBCDT, in 62.7% on MMF, and in 75% on CYC ( = 0.03); the dose of oral prednisone was lower in the IBCDT group (mean ± SD 2.9 ± 5.0 mg/dl) than MMF (10.5 ± 8.0 mg/d, < 0.01) or CYC group (7.5 ± 9.0 mg/d, < 0.01). Mean follow-up after treatment was 44.5 months (interquartile range [IQR] 36-120 months), 48.6 months (IQR 36-120 months), and 45.3 (IQR 36-120 months) for IBCDT, MMF, and CYC, respectively. At their last follow-up visit, we observed no significant differences in proteinuria and serum creatinine, nor in the frequency of new flares among the 3 groups.
In biopsy-proven LN, the IBCDT without further immunosuppressive maintenance therapy was shown to be as effective as conventional regimen of MMF or CYC followed by >3-year maintenance either MMF or AZA regimen. Moreover, the use of IBCDT was associated with a marked reduction of glucocorticoid cumulative dose.
我们旨在研究与活检证实的狼疮性肾炎(LN)的标准治疗相比,强化B细胞清除诱导疗法(IBCDT)在不进行免疫抑制维持治疗方案时的安全性和有效性。
30例患者接受IBCDT治疗(每周1次利妥昔单抗[RTX]375mg/m²,共4次,1个月和2个月后各追加2剂;2次静脉输注10mg/kg环磷酰胺[CYC],3次甲泼尼龙冲击治疗),随后口服泼尼松(至第3个月减至5mg/d)。未给予免疫抑制维持治疗。选择30例LN分级和年龄匹配的患者作为对照:20例接受3次甲泼尼龙冲击治疗,随后口服泼尼松和霉酚酸酯(MMF)2至3g/d,而10例接受欧洲狼疮环磷酰胺方案。MMF(1 - 2g/日)或硫唑嘌呤(AZA,1 - 2mg/kg/日)作为维持治疗>3年。
12个月时,IBCDT组93%的患者实现完全肾脏缓解,MMF组为62.7%,CYC组为75%(P = 0.03);IBCDT组口服泼尼松剂量(均值±标准差2.9±5.0mg/dl)低于MMF组(10.5±8.0mg/d,P < 0.01)或CYC组(7.5±9.0mg/d,P < 0.01)。治疗后平均随访时间IBCDT组为44.5个月(四分位数间距[IQR]36 - 120个月),MMF组为48.6个月(IQR 36 - 120个月),CYC组为45.3个月(IQR 36 - 120个月)。在最后一次随访时,我们观察到3组之间在蛋白尿、血清肌酐以及新发作频率方面无显著差异。
在活检证实的LN中,未进行进一步免疫抑制维持治疗的IBCDT与MMF或CYC常规方案后使用MMF或AZA方案维持治疗>3年的效果相当。此外,IBCDT的使用与糖皮质激素累积剂量的显著降低相关。