Departments of Medicine and Anesthesia, Cardiovascular Research Institute, University of California, San Francisco, CA, USA.
Division of Pulmonary and Critical Care Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Lancet Respir Med. 2021 Aug;9(8):933-936. doi: 10.1016/S2213-2600(21)00105-3. Epub 2021 Apr 27.
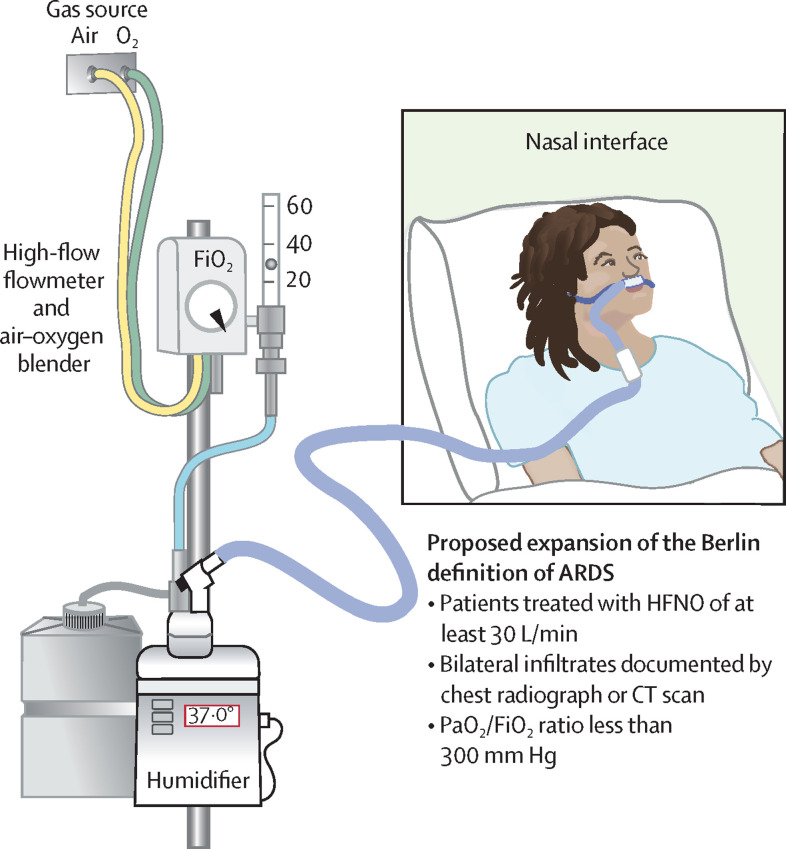
The 2012 Berlin definition of acute respiratory distress syndrome (ARDS) provided validated support for three levels of initial arterial hypoxaemia that correlated with mortality in patients receiving ventilatory support. Since 2015, high-flow nasal oxygen (HFNO) has become widely used as an effective therapeutic support for acute respiratory failure, most recently in patients with severe COVID-19. We propose that the Berlin definition of ARDS be broadened to include patients treated with HFNO of at least 30 L/min who fulfil the other criteria for the Berlin definition of ARDS. An expanded definition would make the diagnosis of ARDS more widely applicable, allowing patients at an earlier stage of the syndrome to be recognised, independent of the need for endotracheal intubation or positive-pressure ventilation, with benefits for the testing of early interventions and the study of factors associated with the course of ARDS. We identify key questions that could be addressed in refining an expanded definition of ARDS, the implementation of which could lead to improvements in clinical practice and clinical outcomes for patients.
2012 年柏林急性呼吸窘迫综合征(ARDS)定义为接受通气支持治疗的患者存在三种初始低氧血症,与死亡率相关,该定义为三种初始低氧血症提供了验证支持。自 2015 年以来,高流量鼻氧(HFNO)已广泛用作急性呼吸衰竭的有效治疗支持,最近在严重 COVID-19 患者中也得到了应用。我们建议将 ARDS 的柏林定义扩大,纳入至少接受 30L/minHFNO 治疗且符合 ARDS 柏林定义其他标准的患者。扩大定义将使 ARDS 的诊断更广泛适用,使处于综合征早期阶段的患者能够得到识别,而无需进行气管插管或正压通气,从而有利于早期干预的测试和与 ARDS 病程相关因素的研究。我们确定了在细化 ARDS 扩展定义时可以解决的关键问题,实施该定义可能会改善患者的临床实践和临床结果。