Department of Emergency and Critical Care Medicine, Nagoya University Graduate School of Medicine, Nagoya, Japan.
Department of Emergency Medicine, Northwell Health, NY, NY, United States of America.
PLoS One. 2021 Apr 30;16(4):e0251030. doi: 10.1371/journal.pone.0251030. eCollection 2021.
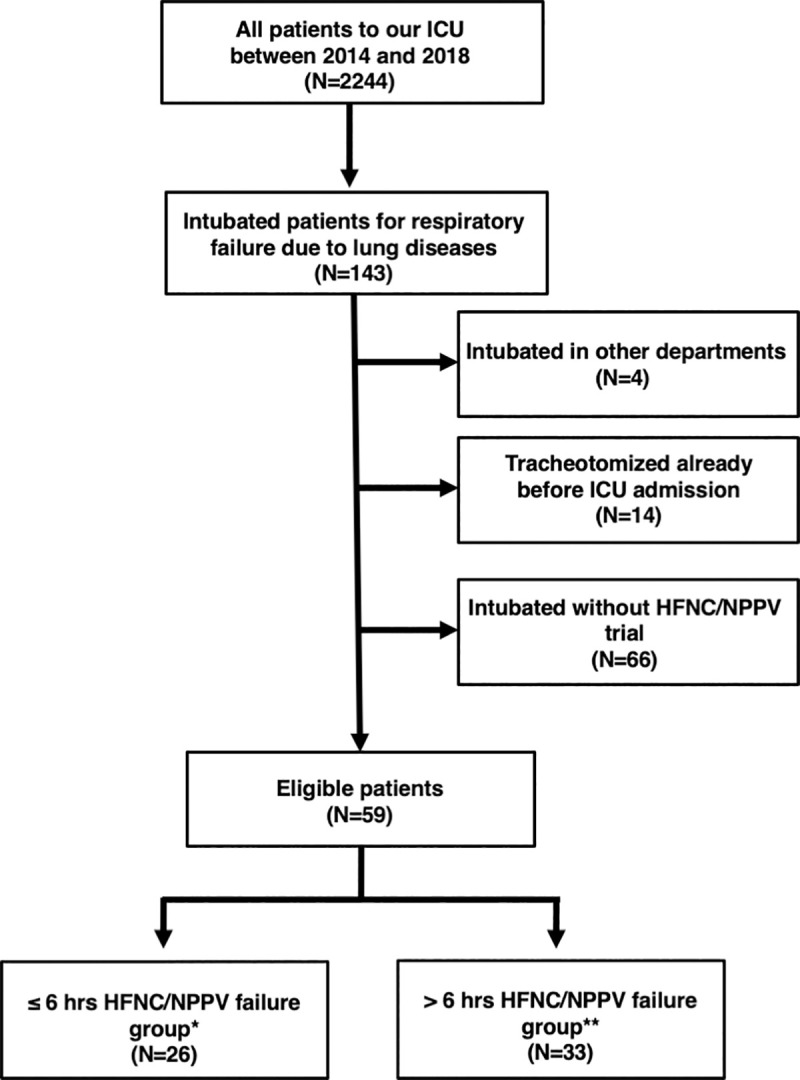
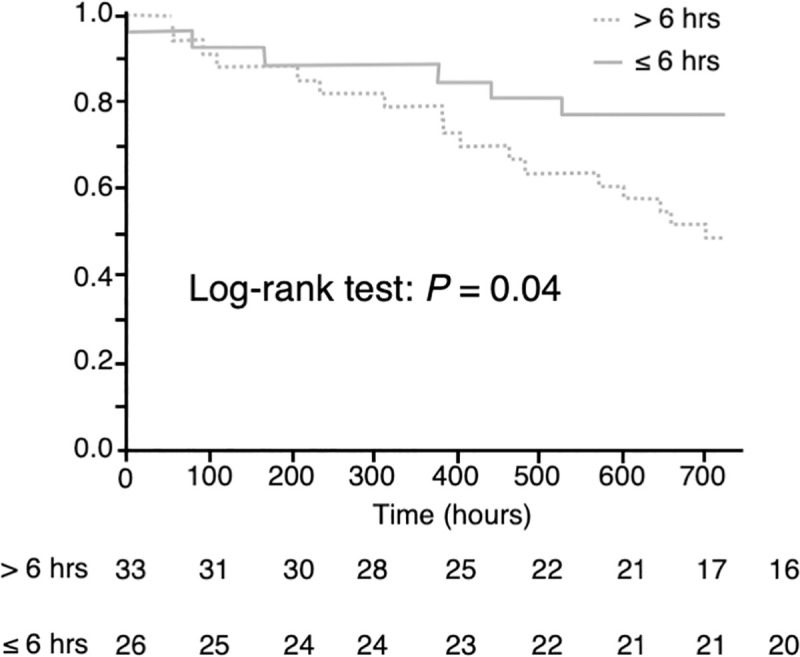
A previous study has shown that late failure (> 48 hours) of high-flow nasal cannula (HFNC) was associated with intensive care unit (ICU) mortality. The aim of this study was to investigate whether failure of non-invasive respiratory support, including HFNC and non-invasive positive pressure ventilation (NPPV), was also associated with the risk of mortality even if it occurs in the earlier phase. We retrospectively analyzed 59 intubated patients for acute respiratory failure due to lung diseases between April 2014 and June 2018. We divided the patients into 2 groups according to the time from starting non-invasive ventilatory support until their intubation: ≤ 6 hours failure and > 6 hours failure group. We evaluated the differences in the ICU mortality between these two groups. The multivariate logistic regression analysis showed the highest mortality in the > 6 hours failure group as compared to the ≤ 6 hours failure group, with a statistically significant difference (p < 0.01). It was also associated with a statistically significant increased 30-day mortality and decreased ventilator weaning rate. The ICU mortality in patients with acute respiratory failure caused by lung diseases was increased if the time until failure of HFNC and NPPV was more than 6 hours.
先前的一项研究表明,高流量鼻导管(HFNC)治疗失败(>48 小时)与重症监护病房(ICU)死亡率相关。本研究旨在探究非侵入性呼吸支持(包括 HFNC 和无创正压通气(NPPV))的治疗失败是否也与死亡率相关,即使它发生在早期阶段。我们回顾性分析了 2014 年 4 月至 2018 年 6 月期间因肺部疾病导致急性呼吸衰竭而插管的 59 例患者。我们根据开始非侵入性通气支持到插管的时间将患者分为两组:≤6 小时失败组和>6 小时失败组。我们评估了两组患者在 ICU 死亡率方面的差异。多变量逻辑回归分析显示,与≤6 小时失败组相比,>6 小时失败组的死亡率更高,差异具有统计学意义(p<0.01)。此外,>6 小时失败组患者的 30 天死亡率增加,通气机撤机率降低,差异具有统计学意义。HFNC 和 NPPV 治疗失败时间超过 6 小时,肺部疾病导致急性呼吸衰竭患者的 ICU 死亡率增加。