Department of Respiratory Medicine, Nagoya University Graduate School of Medicine, Nagoya, Japan.
Pulmonary, Critical Care and Sleep Medicine Section, Department of Internal Medicine, Yale University School of Medicine, New Haven, United States of America.
Nagoya J Med Sci. 2020 May;82(2):301-313. doi: 10.18999/nagjms.82.2.301.
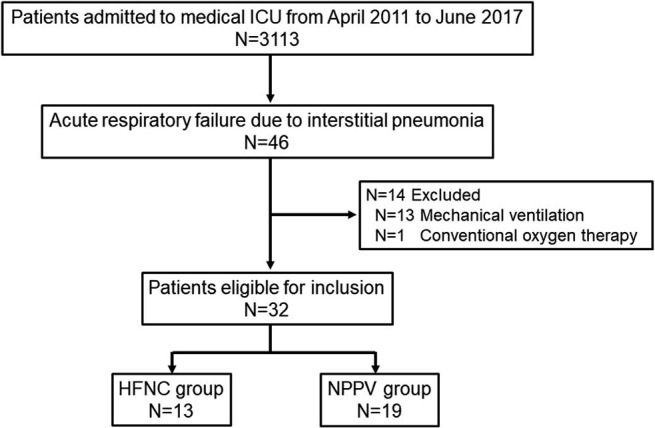
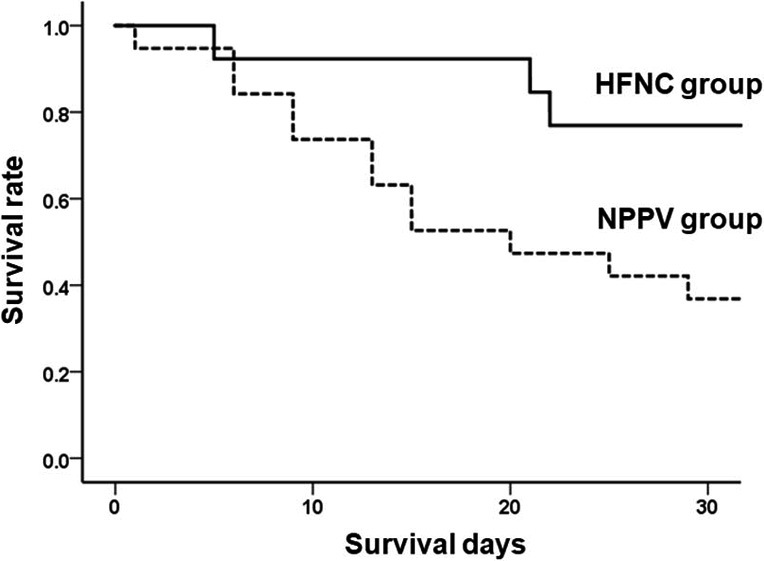
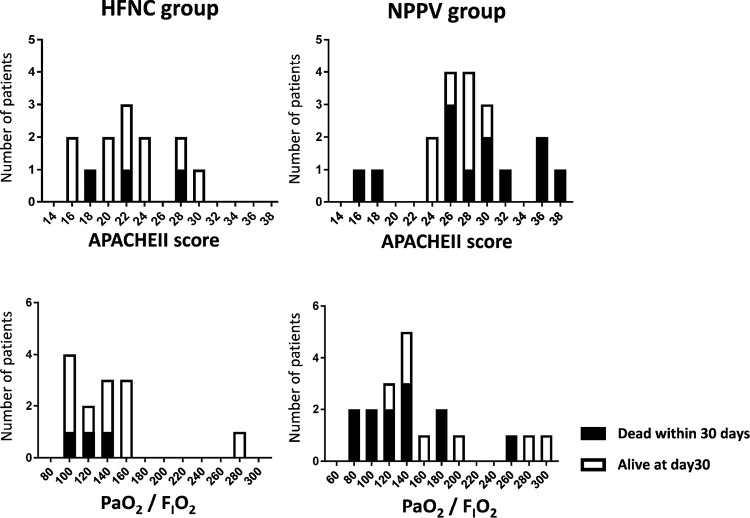
High-flow nasal cannula (HFNC) oxygen is a therapy that has demonstrated survival benefits in acute respiratory failure (ARF). However, the role of HFNC in ARF due to interstitial pneumonia (IP) is unknown. The aim of this study was to compare the effects of HFNC therapy and non-invasive positive pressure ventilation (NPPV) in ARF due to IP. This retrospective observational study included 32 patients with ARF due to IP who were treated with HFNC (n = 13) or NPPV (n = 19). The clinical characteristics, intubation rate and 30-day mortality were analyzed and compared between the HFNC group and the NPPV group. Predictors of 30-day mortality were evaluated using a logistic regression model. HFNC group showed higher mean arterial blood pressure (median 92 mmHg; HFNC group vs 74 mmHg; NPPV group) and lower APACHEII score (median 22; HFNC group vs 27; NPPV group) than NPPV group. There was no significant difference in the intubation rate at day 30 between the HFNC group and the NPPV group (8% vs 37%: p = 0.069); the mortality rate at 30 days was 23% and 63%, respectively. HFNC therapy was a significant determinant of 30-day mortality in univariate analysis, and was confirmed to be an independent significant determinant of 30-day mortality in multivariate analysis (odds ratio, 0.148; 95% confidence interval, 0.025-0.880; p = 0.036). Our findings suggest that HFNC therapy can be a possible option for respiratory management in ARF due to IP. The results observed here warrant further investigation of HFNC therapy in randomized control trials.
高流量鼻导管(HFNC)氧疗在急性呼吸衰竭(ARF)中已被证明具有生存获益。然而,HFNC 在间质性肺炎(IP)所致 ARF 中的作用尚不清楚。本研究旨在比较 HFNC 治疗和无创正压通气(NPPV)在 IP 所致 ARF 中的疗效。本回顾性观察性研究纳入了 13 例接受 HFNC 治疗和 19 例接受 NPPV 治疗的 IP 所致 ARF 患者。分析并比较了 HFNC 组和 NPPV 组患者的临床特征、插管率和 30 天死亡率。使用 logistic 回归模型评估了 30 天死亡率的预测因素。HFNC 组患者的平均动脉血压(中位数 92mmHg;HFNC 组比 NPPV 组 74mmHg)和急性生理与慢性健康状况评分系统 II(APACHE II)评分(中位数 22;HFNC 组比 NPPV 组 27)均高于 NPPV 组。HFNC 组和 NPPV 组患者在第 30 天的插管率无显著差异(8%比 37%:p=0.069);30 天死亡率分别为 23%和 63%。单因素分析显示,HFNC 治疗是 30 天死亡率的显著预测因素,多因素分析也证实 HFNC 治疗是 30 天死亡率的独立显著预测因素(比值比,0.148;95%置信区间,0.025-0.880;p=0.036)。本研究结果表明,HFNC 治疗可能是 IP 所致 ARF 呼吸管理的一种选择。需要进一步开展随机对照试验来研究 HFNC 治疗。