Department of International Health, Johns Hopkins Bloomberg School of Public Health, 415 N Washington Street, Floor 5, Baltimore, MD, 21231, USA.
International Vaccine Access Center, Johns Hopkins Bloomberg School of Public Health, Baltimore, USA.
BMC Public Health. 2021 May 1;21(1):841. doi: 10.1186/s12889-021-10849-y.
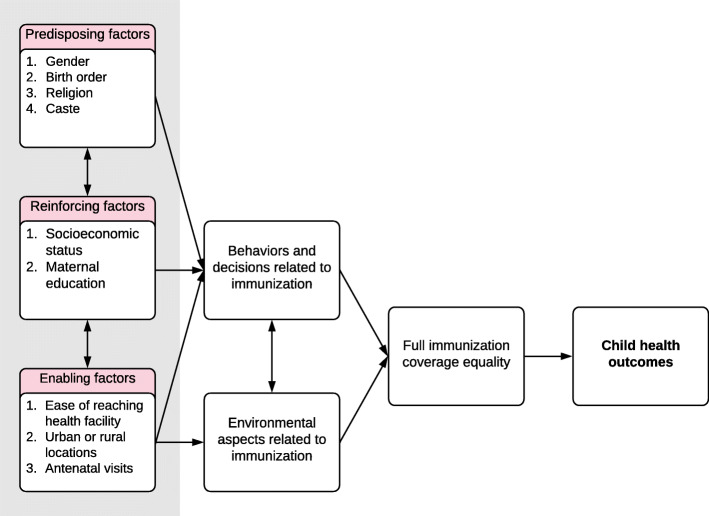
India has made substantial progress in improving child health in recent years. However, the country continues to account for a large number of vaccine preventable child deaths. We estimated wealth-related full immunization inequalities in India. We also calculated the degree to which predisposing, reinforcing, and enabling factors contribute to these inequalities.
We used data from the two rounds of a large nationally representative survey done in all states in India in 2005-06 (n = 9582) and 2015-16 (n = 49,284). Full immunization status was defined as three doses of diphtheria-tetanus-pertussis vaccine, three doses of polio vaccine, one dose of Bacillus Calmette-Guérin vaccine, and one dose of measles vaccine in children 12-23 months. We compared full immunization coverage by wealth quintiles using descriptive statistics. We calculated concentration indices for full immunization coverage at the national and state levels. Using predisposing, reinforcing, and enabling factors associated with full immunization status identified from the literature, we applied a generalized linear model (GLM) framework with a binomial distribution and an identity link to decompose the concentration index.
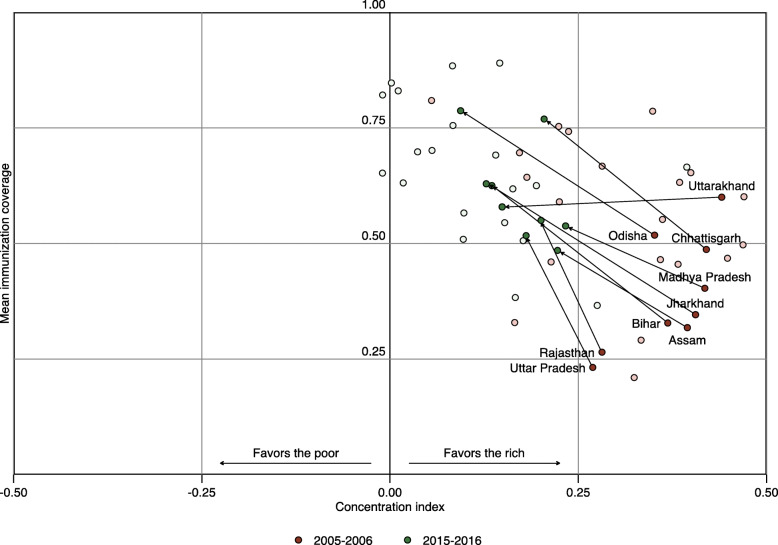
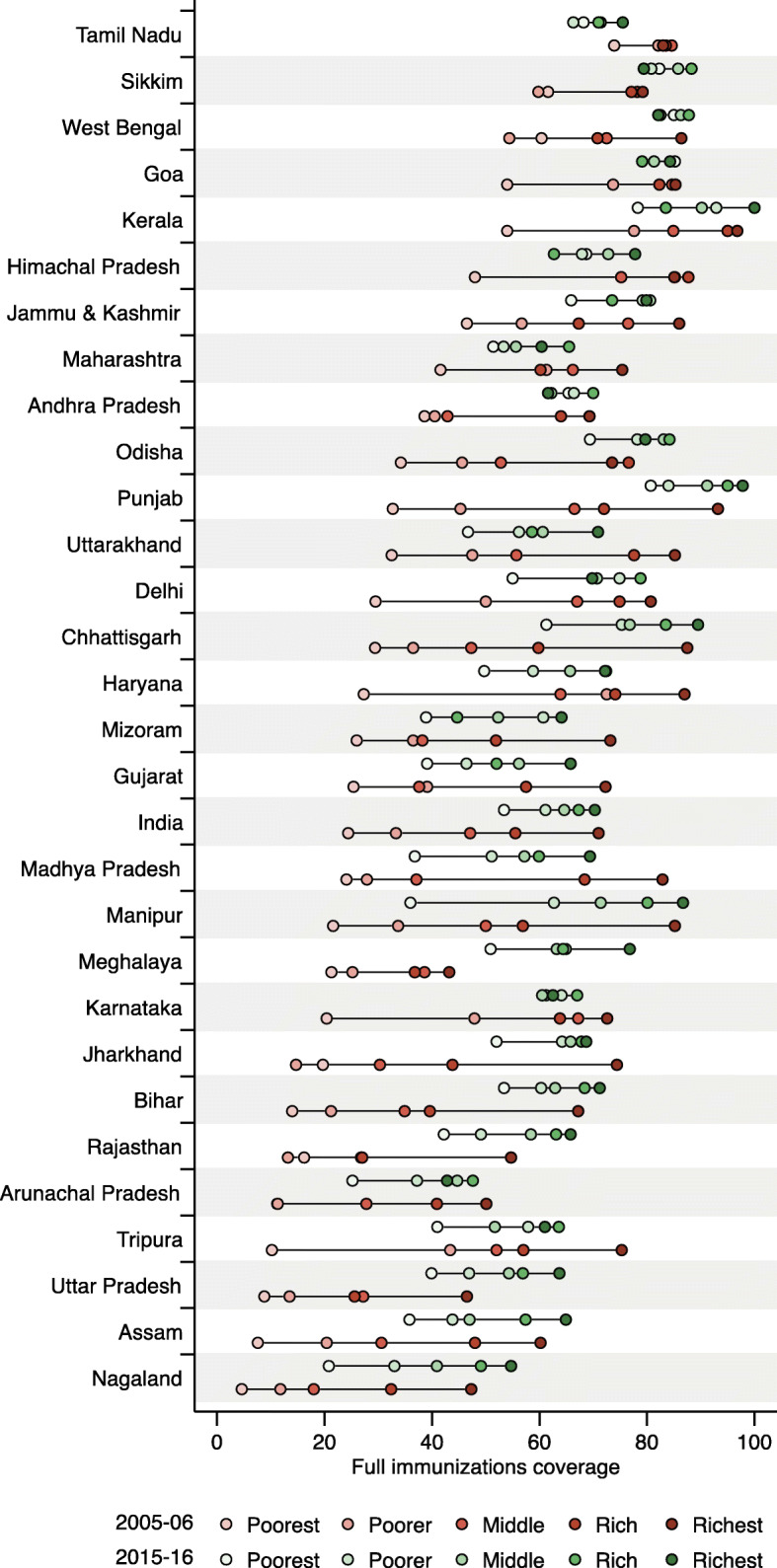
National full immunization coverage increased from 43.65% in 2005-06 to 62.46% in 2015-16. Overall, full immunization coverage in both 2005-06 and 2015-16 in all states was lowest in children from poorer households and improved with increasing socioeconomic status. The national concentration index decreased from 0.36 to 0.13 between the two study periods, indicating a reduction in poor-rich inequality. Similar reductions were observed for most states, except in states where inequalities were already minimal (i.e., Tamil Nadu) and in some northeastern states (i.e., Meghalaya and Manipur). In 2005-06, the contributors to wealth-related full immunization inequality were antenatal care, maternal education, and socioeconomic status. The same factors contributed to full immunization inequality in 2015-16 in addition to difficulty reaching a health facility.
Immunization coverage and wealth-related equality have improved nationally and in most states over the last decade in India. Targeted, context-specific interventions could help address overall wealth-related full immunization inequalities. Intensified government efforts could help in this regard, particularly in high-focus states where child mortality remains high.
近年来,印度在改善儿童健康方面取得了重大进展。然而,该国仍然有大量疫苗可预防的儿童死亡。我们评估了印度与财富相关的完全免疫不平等。我们还计算了促成这些不平等的倾向因素、强化因素和促成因素的程度。
我们使用了 2005-06 年(n=9582)和 2015-16 年(n=49284)两轮在印度所有邦进行的一项大型全国代表性调查的数据。完全免疫状态定义为 12-23 个月儿童接种三剂白喉、破伤风、百日咳疫苗、三剂脊髓灰质炎疫苗、一剂卡介苗和一剂麻疹疫苗。我们使用描述性统计比较了按财富五分位数划分的完全免疫覆盖率。我们计算了国家和邦层面完全免疫覆盖率的集中指数。根据文献中确定的与完全免疫状态相关的倾向因素、强化因素和促成因素,我们应用具有二项分布和恒等链接的广义线性模型(GLM)框架对集中指数进行了分解。
全国完全免疫覆盖率从 2005-06 年的 43.65%增加到 2015-16 年的 62.46%。总体而言,在 2005-06 年和 2015-16 年,所有邦的最贫困家庭儿童的完全免疫覆盖率最低,随着社会经济地位的提高而提高。全国集中指数从两个研究期间的 0.36 下降到 0.13,表明贫富不平等有所减少。除了不平等已经很小的邦(即泰米尔纳德邦)和一些东北部邦(即梅加拉亚邦和曼尼普尔邦)外,大多数邦的情况都有类似的改善。在 2005-06 年,产前护理、产妇教育和社会经济地位是造成与财富相关的完全免疫不平等的原因。在 2015-16 年,除了难以到达医疗机构外,同样的因素也导致了完全免疫的不平等。
在过去十年中,印度在全国和大多数邦的免疫覆盖率和与财富相关的平等都有所提高。有针对性的、具体情况的干预措施可以帮助解决与财富相关的完全免疫整体不平等。政府的大力加强可以在这方面提供帮助,特别是在儿童死亡率仍然很高的重点邦。