School of Public Health and Family Medicine, Health Policy and Systems Division, University of Cape Town, Cape Town, South Africa.
Kenya Medical Research Institute (KEMRI)-Wellcome-Trust Research Programme, Kilifi, Kenya.
Int J Equity Health. 2021 May 1;20(1):112. doi: 10.1186/s12939-021-01447-w.
The World Health Organisation framed responsiveness, fair financing and equity as intrinsic goals of health systems. However, of the three, responsiveness received significantly less attention. Responsiveness is essential to strengthen systems' functioning; provide equitable and accountable services; and to protect the rights of citizens. There is an urgency to make systems more responsive, but our understanding of responsiveness is limited. We therefore sought to map existing evidence on health system responsiveness.
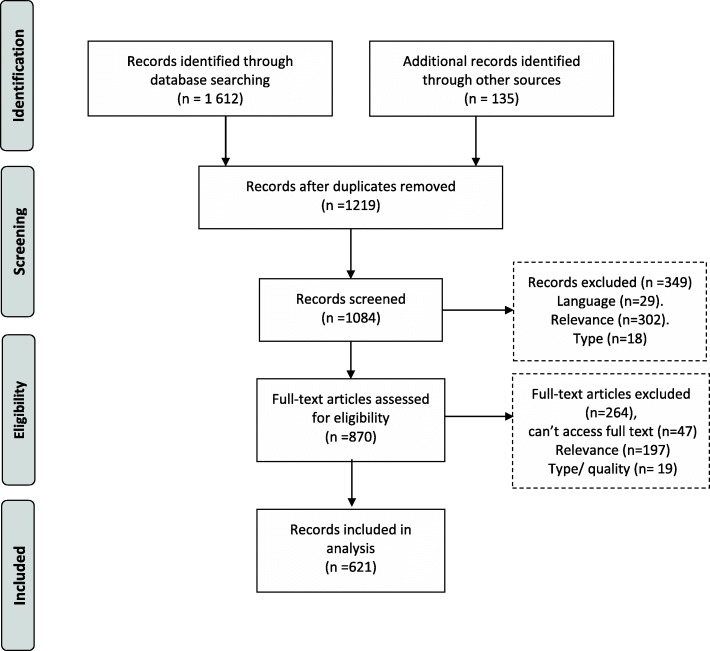
A mixed method systemized evidence mapping review was conducted. We searched PubMed, EbscoHost, and Google Scholar. Published and grey literature; conceptual and empirical publications; published between 2000 and 2020 and English language texts were included. We screened titles and abstracts of 1119 publications and 870 full texts.
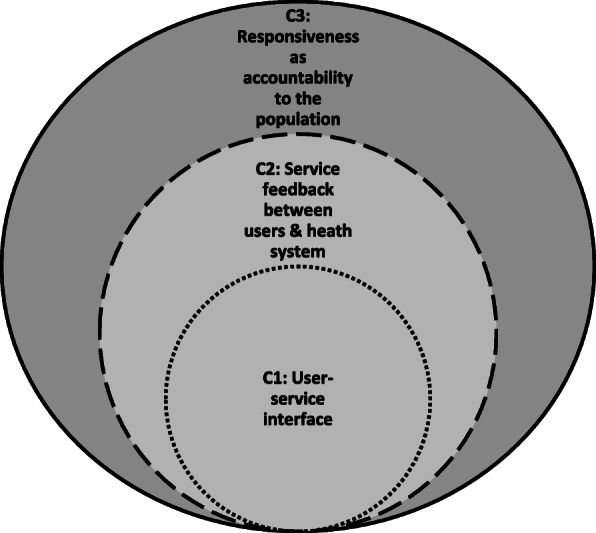
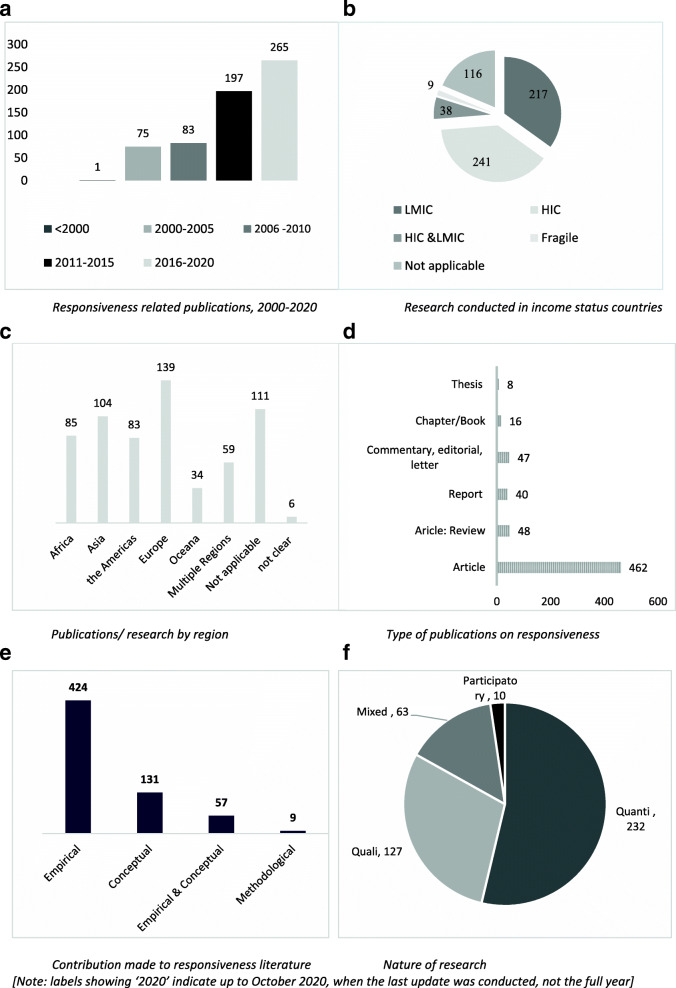
Six hundred twenty-one publications were included in the review. Evidence mapping shows substantially more publications between 2011 and 2020 (n = 462/621) than earlier periods. Most of the publications were from Europe (n = 139), with more publications relating to High Income Countries (n = 241) than Low-to-Middle Income Countries (n = 217). Most were empirical studies (n = 424/621) utilized quantitative methodologies (n = 232), while qualitative (n = 127) and mixed methods (n = 63) were more rare. Thematic analysis revealed eight primary conceptualizations of 'health system responsiveness', which can be fitted into three dominant categorizations: 1) unidirectional user-service interface; 2) responsiveness as feedback loops between users and the health system; and 3) responsiveness as accountability between public and the system.
This evidence map shows a substantial body of available literature on health system responsiveness, but also reveals evidential gaps requiring further development, including: a clear definition and body of theory of responsiveness; the implementation and effectiveness of feedback loops; the systems responses to this feedback; context-specific mechanism-implementation experiences, particularly, of LMIC and fragile-and conflict affected states; and responsiveness as it relates to health equity, minority and vulnerable populations. Theoretical development is required, we suggest separating ideas of services and systems responsiveness, applying a stronger systems lens in future work. Further agenda-setting and resourcing of bridging work on health system responsiveness is suggested.
世界卫生组织将反应性、公平筹资和公平作为卫生系统的内在目标。然而,在这三个目标中,反应性受到的关注明显较少。反应性对于加强系统的功能、提供公平和负责任的服务以及保护公民的权利至关重要。现在迫切需要使系统更具反应性,但我们对反应性的理解有限。因此,我们试图绘制现有卫生系统反应性证据图。
进行了一项混合方法系统的证据映射审查。我们搜索了 PubMed、EbscoHost 和 Google Scholar。纳入了已发表和灰色文献;概念和经验出版物;发表于 2000 年至 2020 年期间的英文文本。我们筛选了 1119 篇出版物的标题和摘要以及 870 篇全文。
有 621 篇出版物纳入了本综述。证据图显示,2011 年至 2020 年期间的出版物数量大大增加(n=462/621),而早期时期的出版物数量较少。大多数出版物来自欧洲(n=139),高收入国家(n=241)的出版物数量多于中低收入国家(n=217)。大多数是实证研究(n=424/621),采用定量方法(n=232),而定性(n=127)和混合方法(n=63)则较少。主题分析揭示了“卫生系统反应性”的八个主要概念化,可以归入三个主要分类:1)单向用户-服务接口;2)用户与卫生系统之间的反馈循环的反应性;3)公共部门与系统之间的问责制的反应性。
本证据图显示了大量关于卫生系统反应性的现有文献,但也揭示了需要进一步发展的证据空白,包括:反应性的明确定义和理论体系;反馈循环的实施和有效性;系统对这种反馈的反应;特定于上下文的机制-实施经验,特别是中低收入国家和脆弱和冲突影响国家;以及反应性与卫生公平、少数民族和弱势群体的关系。需要进行理论发展,我们建议将服务和系统反应性的概念分开,在未来的工作中应用更强的系统视角。建议为卫生系统反应性的桥接工作制定进一步的议程和资源配置。