Ram-Mohan Nikhil, Kim David, Zudock Elizabeth J, Hashemi Marjan M, Tjandra Kristel C, Rogers Angela J, Blish Catherine A, Nadeau Kari C, Newberry Jennifer A, Quinn James V, O'Hara Ruth, Ashley Euan, Nguyen Hien, Jiang Lingxia, Hung Paul, Blomkalns Andra L, Yang Samuel
Department of Emergency Medicine, Stanford University School of Medicine, Palo Alto, California, USA.
Department of Medicine-Pulmonary, Allergy & Critical Care Medicine, Stanford University School of Medicine, Palo Alto, California, USA.
Clin Infect Dis. 2022 Jan 29;74(2):218-226. doi: 10.1093/cid/ciab394.
The determinants of coronavirus disease 2019 (COVID-19) disease severity and extrapulmonary complications (EPCs) are poorly understood. We characterized relationships between severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) RNAemia and disease severity, clinical deterioration, and specific EPCs.
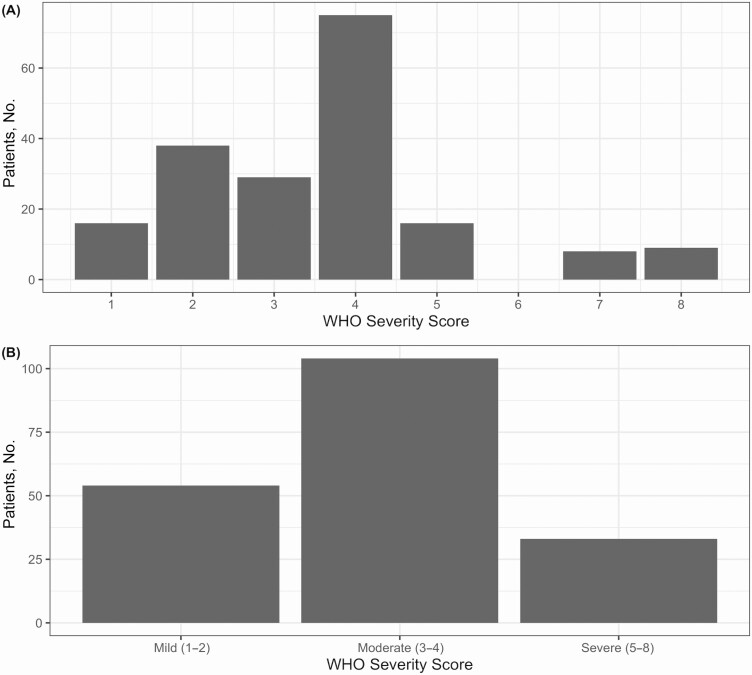
We used quantitative and digital polymerase chain reaction (qPCR and dPCR) to quantify SARS-CoV-2 RNA from plasma in 191 patients presenting to the emergency department with COVID-19. We recorded patient symptoms, laboratory markers, and clinical outcomes, with a focus on oxygen requirements over time. We collected longitudinal plasma samples from a subset of patients. We characterized the role of RNAemia in predicting clinical severity and EPCs using elastic net regression.
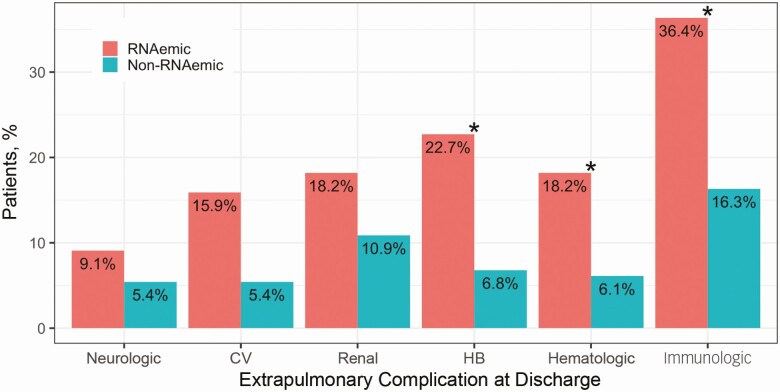
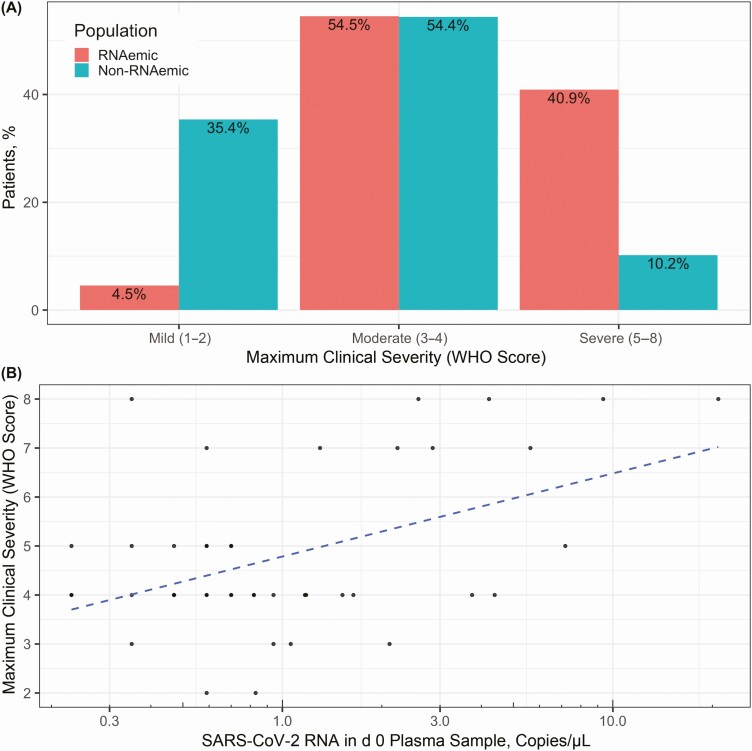
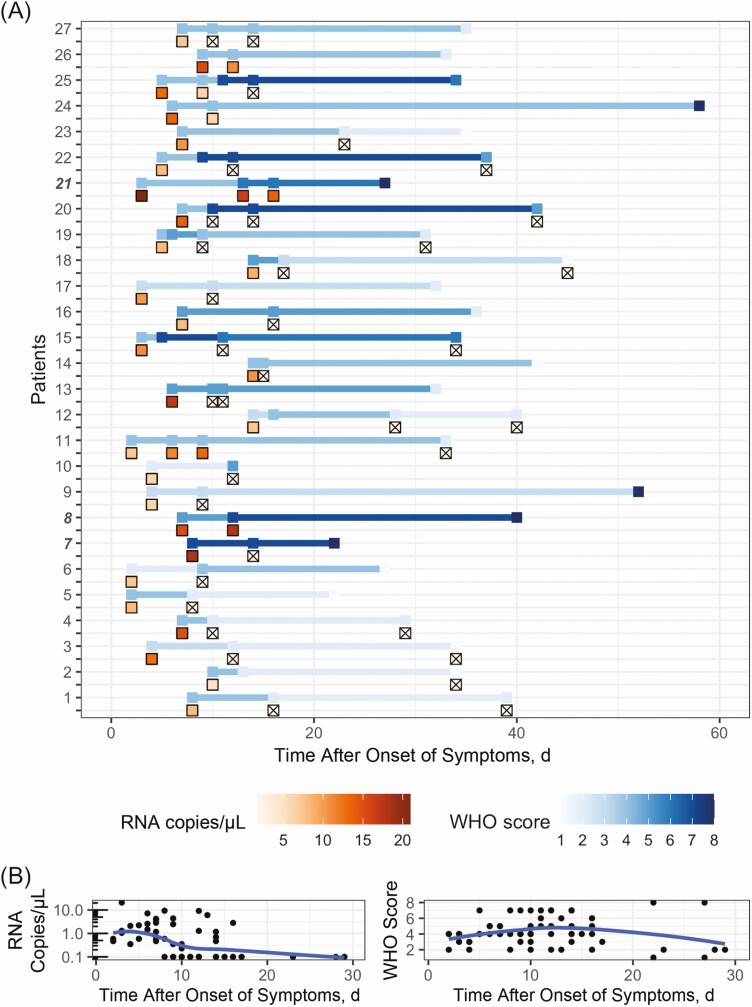
Of SARS-CoV-2-positive patients, 23.0% (44 of 191) had viral RNA detected in plasma by dPCR, compared with 1.4% (2 of 147) by qPCR. Most patients with serial measurements had undetectable RNAemia within 10 days of symptom onset, reached maximum clinical severity within 16 days, and symptom resolution within 33 days. Initially RNAemic patients were more likely to manifest severe disease (odds ratio, 6.72 [95% confidence interval, 2.45-19.79]), worsening of disease severity (2.43 [1.07-5.38]), and EPCs (2.81 [1.26-6.36]). RNA loads were correlated with maximum severity (r = 0.47 [95% confidence interval, .20-.67]).
dPCR is more sensitive than qPCR for the detection of SARS-CoV-2 RNAemia, which is a robust predictor of eventual COVID-19 severity and oxygen requirements, as well as EPCs. Because many COVID-19 therapies are initiated on the basis of oxygen requirements, RNAemia on presentation might serve to direct early initiation of appropriate therapies for the patients most likely to deteriorate.
2019冠状病毒病(COVID-19)疾病严重程度和肺外并发症(EPCs)的决定因素尚不清楚。我们对严重急性呼吸综合征冠状病毒2(SARS-CoV-2)病毒血症与疾病严重程度、临床恶化及特定EPCs之间的关系进行了特征描述。
我们使用定量和数字聚合酶链反应(qPCR和dPCR)对191例因COVID-19到急诊科就诊患者的血浆中SARS-CoV-2 RNA进行定量。我们记录了患者症状、实验室指标和临床结局,重点关注随时间变化的氧气需求情况。我们从一部分患者中收集了纵向血浆样本。我们使用弹性网络回归来描述病毒血症在预测临床严重程度和EPCs中的作用。
在SARS-CoV-2阳性患者中,23.0%(191例中的44例)通过dPCR在血浆中检测到病毒RNA,而通过qPCR检测到的为1.4%(147例中的2例)。大多数进行连续测量的患者在症状出现后10天内病毒血症检测不到,在16天内达到最大临床严重程度,在33天内症状缓解。最初有病毒血症的患者更有可能表现为严重疾病(优势比,6.72 [95%置信区间,2.45 - 19.79])、疾病严重程度恶化(2.43 [1.07 - 5.38])和EPCs(2.81 [1.26 - 6.36])。病毒载量与最大严重程度相关(r = 0.47 [95%置信区间,0.20 - 0.67])。
dPCR在检测SARS-CoV-2病毒血症方面比qPCR更敏感,病毒血症是最终COVID-19严重程度、氧气需求以及EPCs的有力预测指标。由于许多COVID-19治疗是根据氧气需求启动的,就诊时的病毒血症可能有助于指导对最有可能病情恶化的患者尽早开始适当治疗。