Leicester Kidney Lifestyle Team, Department of Health Sciences, University of Leicester, Leicester, UK.
Leicester NIHR Biomedical Research Centre, Leicester, UK.
J Cachexia Sarcopenia Muscle. 2021 Jun;12(3):586-598. doi: 10.1002/jcsm.12705. Epub 2021 May 5.
Sarcopenia, a degenerative and generalized skeletal muscle disorder involving the loss of muscle function and mass, is an under-recognized problem in clinical practice, particularly in chronic kidney disease (CKD). We aimed to investigate the prevalence of sarcopenia in individuals with CKD, its risk factors, and its association with all-cause mortality and progression to end-stage renal disease (ESRD).
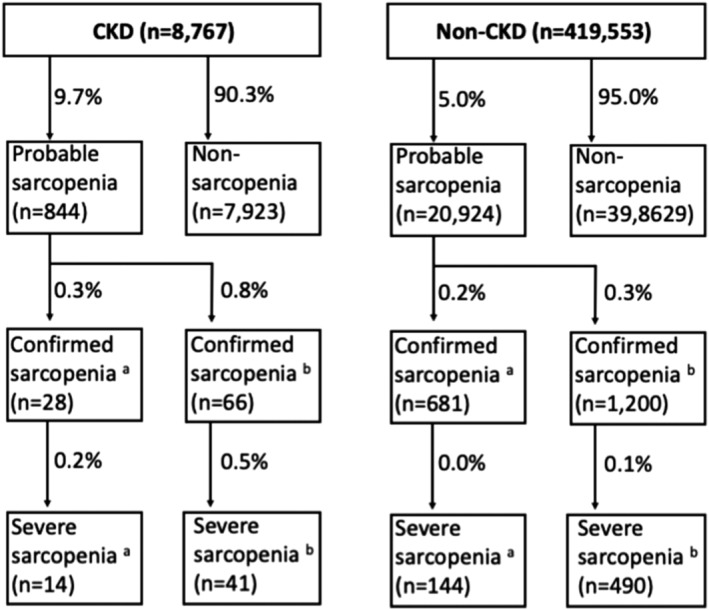
UK Biobank participants were grouped according to the presence of CKD (defined as an estimated glomerular filtration rate <60 mL/min/1.73 m ) and as having probable (low handgrip strength), confirmed (plus low muscle mass), and severe sarcopenia (plus poor physical performance) based on the 2019 European Working Group of Sarcopenia in Older People and Foundation for the National Institutes of Health criteria. Risk factors were explored using logistic regression analysis. Survival models were applied to estimate risk of mortality and ESRD.
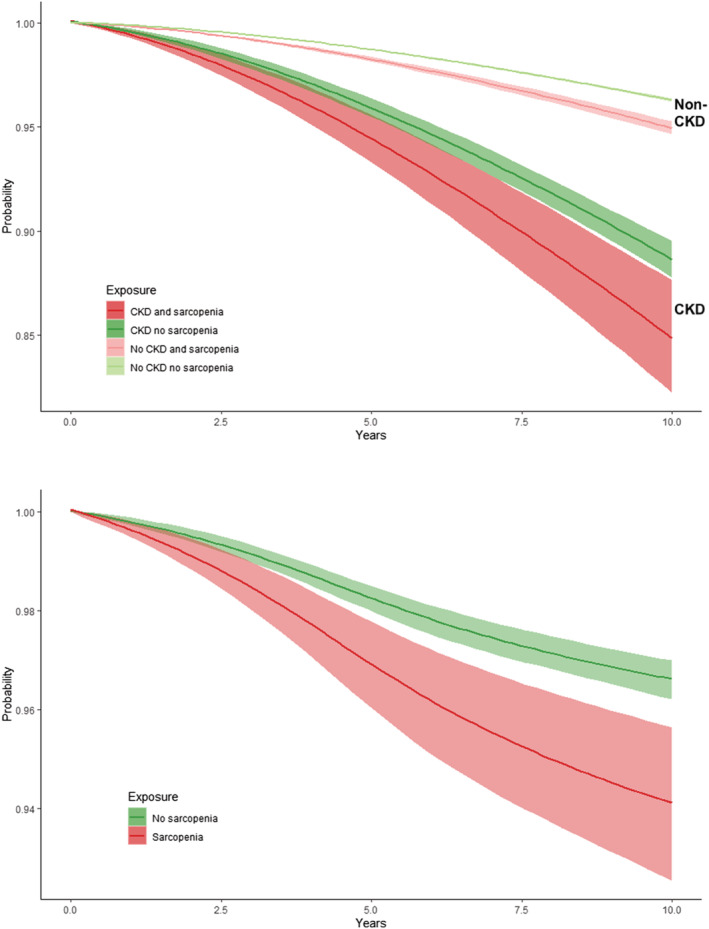
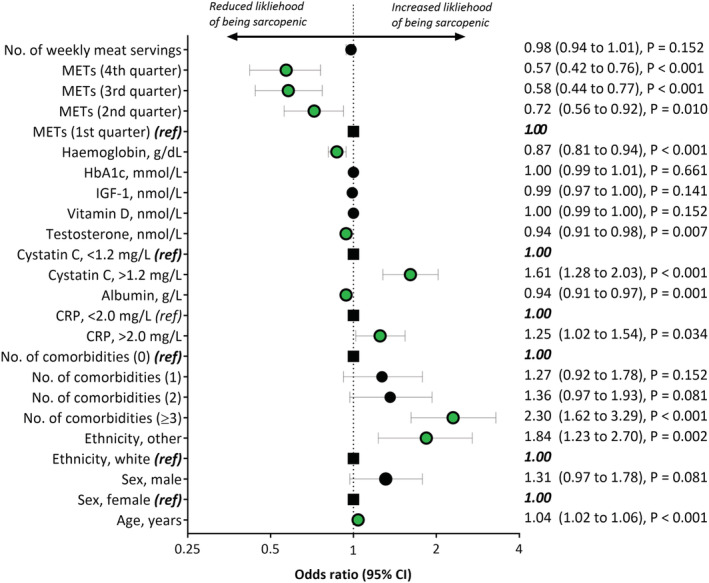
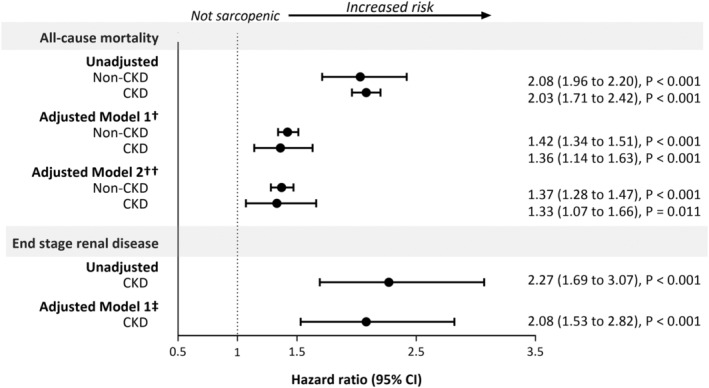
A total of 428 320 participants, of which 8767 individuals with CKD (46% male, aged 62.8 (standard deviation 6.8) years, median estimated glomerular filtration rate 54.5 (interquartile range 49.0-57.7) mL/min/1.72 m ) were included. Probable sarcopenia was present in 9.7% of individuals with CKD compared with 5.0% in those without (P < 0.001). Sarcopenia was associated with being older; inflammation; poorer renal function; and lower serum albumin, total testosterone, and haemoglobin. The largest risk factors for sarcopenia were having three or more comorbidities (odds ratio: 2.30; 95% confidence interval: 1.62 to 3.29; P < 0.001) and physical inactivity: participants in the highest quartile of weekly activity were 43% less likely to have sarcopenia compared to the lowest quartile (odds ratio: 0.57; 0.42 to 0.76; P < 0.001). Participants with CKD and sarcopenia had a 33% (7% to 66%; P = 0.011) higher hazard of mortality compared with individuals without. Sarcopenic CKD individuals had a 10 year survival probability of 0.85 (0.82 to 0.88) compared with 0.89 (0.88 to 0.30) in those without sarcopenia, an absolute difference of 4%. Those with sarcopenia were twice as likely to develop ESRD (hazard ratio: 1.98; 1.45 to 2.70; P < 0.001).
Participants with reduced kidney function are at an increased risk of premature mortality. The presence of sarcopenia increases the risk of mortality and ESRD. Appropriate measurement of sarcopenia should be used to identify at-risk individuals. Interventions such as physical activity should be encouraged to mitigate sarcopenia.
肌少症是一种退行性和全身性的骨骼肌疾病,涉及肌肉功能和质量的丧失,在临床实践中特别是在慢性肾脏病(CKD)中尚未得到充分认识。我们旨在研究 CKD 患者肌少症的患病率、其危险因素,以及其与全因死亡率和进展至终末期肾病(ESRD)的关系。
根据存在 CKD(定义为估计肾小球滤过率<60 mL/min/1.73 m )将 UK Biobank 参与者进行分组,并根据 2019 年欧洲老年人肌肉减少症工作组和美国国立卫生研究院基金会的标准,将可能存在(握力低)、确诊(加上肌肉量低)和严重肌少症(加上身体机能差)的患者分为肌少症组。使用逻辑回归分析探讨危险因素。应用生存模型估计死亡率和 ESRD 的风险。
共纳入 428320 名参与者,其中 8767 名 CKD 患者(46%为男性,年龄 62.8(标准差 6.8)岁,中位估计肾小球滤过率 54.5(四分位间距 49.0-57.7)mL/min/1.72 m )。与无 CKD 者相比(5.0%),CKD 患者中可能存在肌少症者比例更高(9.7%)(P<0.001)。肌少症与年龄较大、炎症、肾功能较差以及血清白蛋白、总睾酮和血红蛋白水平较低有关。肌少症的最大危险因素是有三种或更多种合并症(比值比:2.30;95%置信区间:1.62 至 3.29;P<0.001)和缺乏身体活动:与最低四分位数相比,每周活动量最高四分位数的参与者发生肌少症的可能性低 43%(比值比:0.57;0.42 至 0.76;P<0.001)。与无肌少症者相比,CKD 合并肌少症患者的死亡率风险高 33%(7%至 66%;P=0.011)。肌少症 CKD 患者的 10 年生存率为 0.85(0.82 至 0.88),而无肌少症者为 0.89(0.88 至 0.30),绝对差异为 4%。有肌少症的患者发生 ESRD 的风险高 2 倍(风险比:1.98;1.45 至 2.70;P<0.001)。
肾功能降低的患者过早死亡的风险增加。肌少症的存在增加了死亡率和 ESRD 的风险。应适当测量肌少症以识别高危人群。应鼓励身体活动等干预措施来减轻肌少症。