Institute of Cardiovascular Medicine and Science, Liverpool Heart and Chest Hospital, Liverpool, UK
Heart Center, Jessa Hospital, Hasselt, Belgium.
Heart. 2021 Aug;107(16):1296-1302. doi: 10.1136/heartjnl-2020-318676. Epub 2021 May 5.
Pulmonary vein isolation (PVI) guided by a standardised CLOSE (contiguous optimised lesions) protocol has been shown to increase clinical success after catheter ablation for paroxysmal atrial fibrillation (PAF). This study analysed healthcare utilisation and quality of life (QOL) outcomes from a large multicentre prospective study, measured association between QOL and atrial fibrillation (AF) burden and identified factors associated with lack of QOL improvement.
CLOSE-guided ablation was performed in 329 consecutive patients (age 61.4 years, 60.8% male) with drug-refractory PAF in 17 European centres. QOL was measured at baseline and 12 months post-ablation via Atrial Fibrillation Effect on QualiTy of Life Survey (AFEQT) and EuroQoL EQ-5D-5L questionnaires. All-cause and cardiovascular hospitalisations and cardioversions over 12 months pre-ablation and post-ablation were recorded. Rhythm monitoring included weekly and symptom-driven trans-telephonic monitoring, plus ECG and Holter monitoring at 3, 6 and 12 months. AF burden was defined as the percentage of postblanking tracings with an atrial tachyarrhythmia ≥30 s. Continuous measures across multiple time points were analysed using paired t-tests, and associations between various continuous measures were analysed using independent sample t-tests. Each statistical test used two-sided p values with a significance level of 0.05.
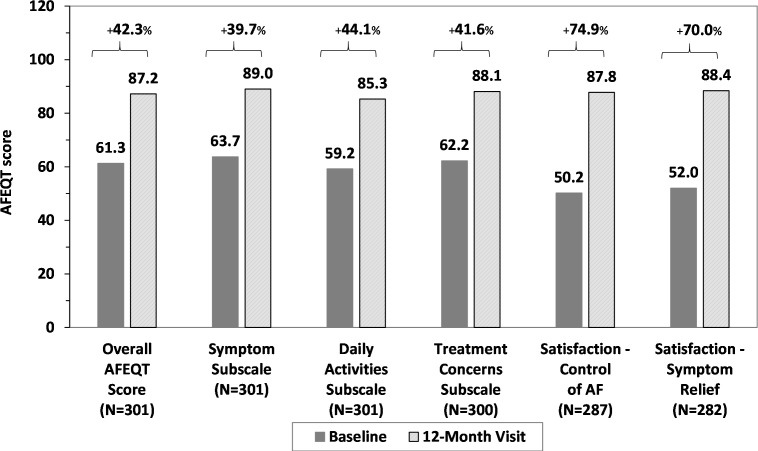
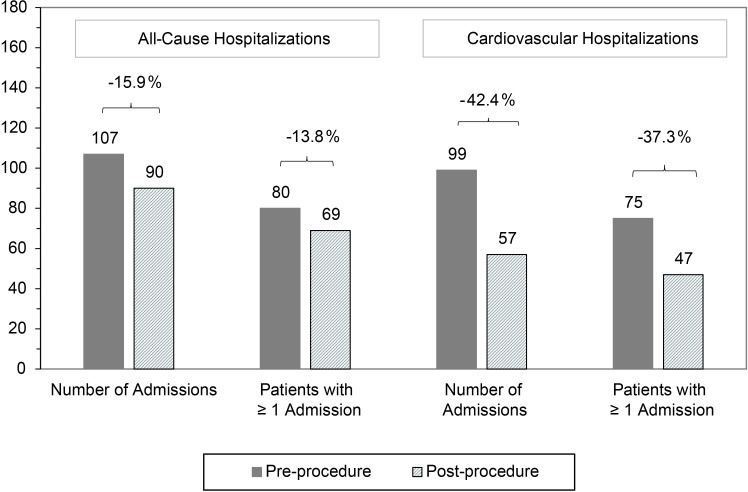
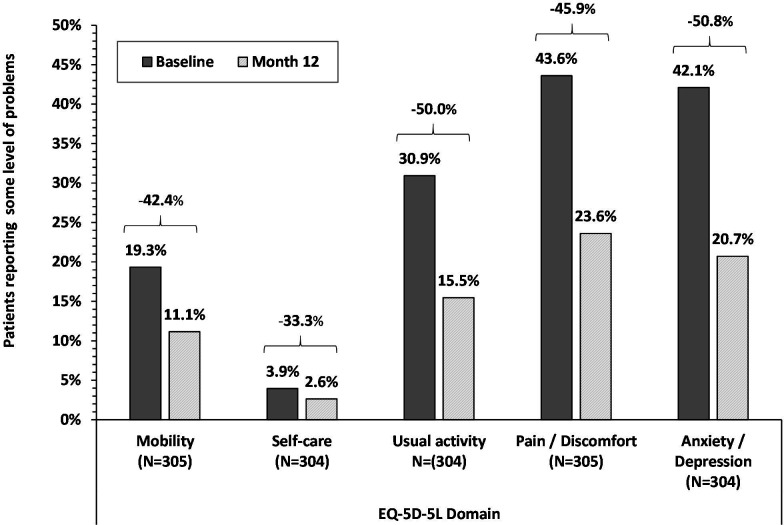
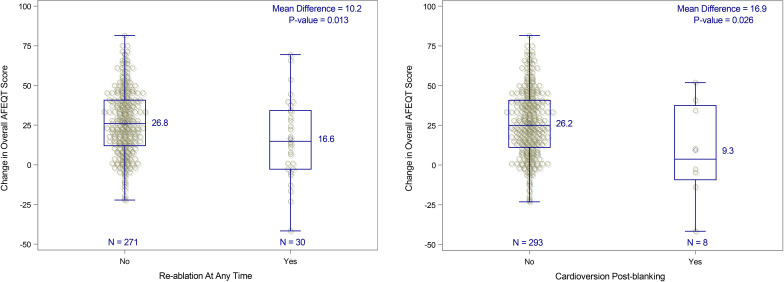
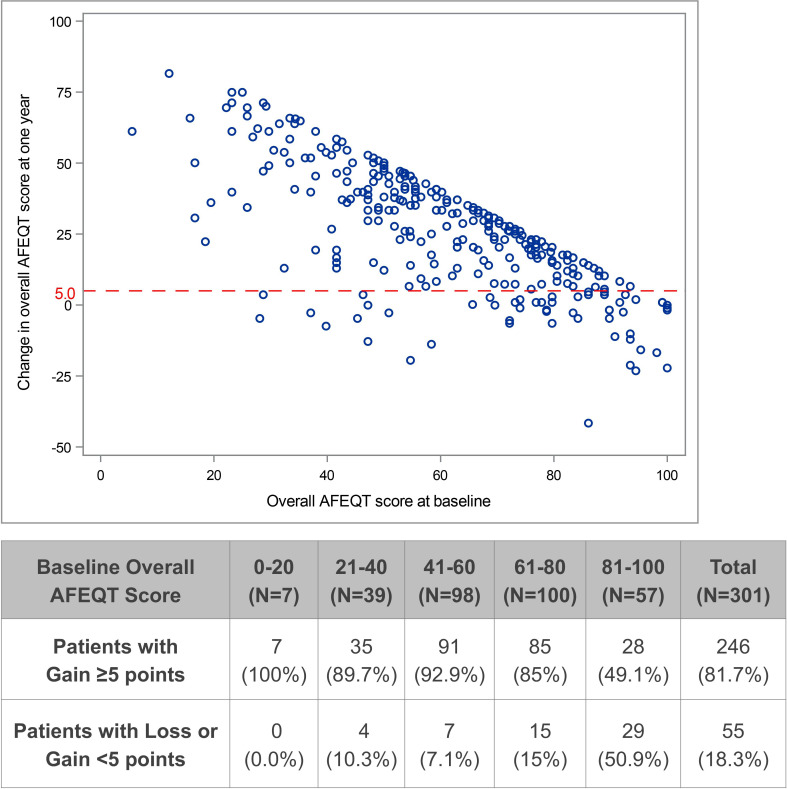
Both QOL instruments showed significant 12-month improvements across all domains: AFEQT score increased 25.1-37.5 points and 33.3%-50.8% fewer patients reporting any problem across EuroQoL EQ-5D-5L domains. Overall, AFEQT improvement was highly associated with AF burden (p=0.009 for <10% vs ≥10% burden, p<0.001 for <20% vs ≥20% burden). Cardiovascular hospitalisations were significantly decreased after ablation (42%, p=0.001). Patients without substantial improvement in AFEQT (55/301, 18.2%) had higher AFEQT and CHADS-VASc scores at baseline, and higher AF burden following PVI.
QOL improved and healthcare utilisation decreased significantly after ablation with a standardised CLOSE protocol. QOL improvement was significantly associated with impairment at baseline and AF burden after ablation.
NCT03062046.
在标准的 CLOSE(连续优化病变)方案指导下进行肺静脉隔离(PVI)已被证明可增加导管消融阵发性心房颤动(PAF)后的临床成功率。本研究通过一项大型多中心前瞻性研究分析了医疗保健的利用情况和生活质量(QOL)结果,测量了 QOL 与心房颤动(AF)负担之间的关联,并确定了与 QOL 改善不足相关的因素。
在 17 个欧洲中心对 329 例药物难治性 PAF 的连续患者(年龄 61.4 岁,60.8%为男性)进行了 CLOSE 引导消融。通过心房颤动对生活质量影响调查(AFEQT)和欧洲五维健康量表(EQ-5D-5L)问卷在基线和消融后 12 个月测量 QOL。记录消融前 12 个月和消融后所有原因和心血管住院和电复律。节律监测包括每周和症状驱动的远程电话监测,以及消融后 3、6 和 12 个月的心电图和动态心电图监测。AF 负担定义为空白后描记中≥30 秒的房性心动过速/心房颤动的百分比。使用配对 t 检验分析多个时间点的连续测量值,使用独立样本 t 检验分析各种连续测量值之间的关联。每个统计检验均使用双侧 p 值,显著性水平为 0.05。
两种 QOL 工具在所有领域均显示出 12 个月的显著改善:AFEQT 评分增加了 25.1-37.5 分,在欧洲五维健康量表(EQ-5D-5L)领域报告任何问题的患者比例减少了 33.3%-50.8%。总体而言,AFEQT 的改善与 AF 负担高度相关(p=0.009,<10%与≥10%的负担,p<0.001,<20%与≥20%的负担)。消融后心血管住院率显著下降(42%,p=0.001)。在 AFEQT 中没有显著改善的患者(55/301,18.2%)在基线时的 AFEQT 和 CHADS-VASc 评分较高,并且在 PVI 后 AF 负担较高。
使用标准的 CLOSE 方案进行消融后,QOL 显著改善,医疗保健利用率降低。QOL 的改善与基线时的损伤和消融后的 AF 负担显著相关。
NCT03062046。