Cardiology, Cardiothoracic Department, University Hospital "Santa Maria della Misericordia", ASUFC, Piazzale Santa Maria della Misericordia 15, 33100 Udine, Italy.
GenesisCare, 3/140 Mounts Bay Rd, Perth, Western Australia, Australia.
Eur Heart J. 2021 Jul 21;42(28):2745-2760. doi: 10.1093/eurheartj/ehab221.
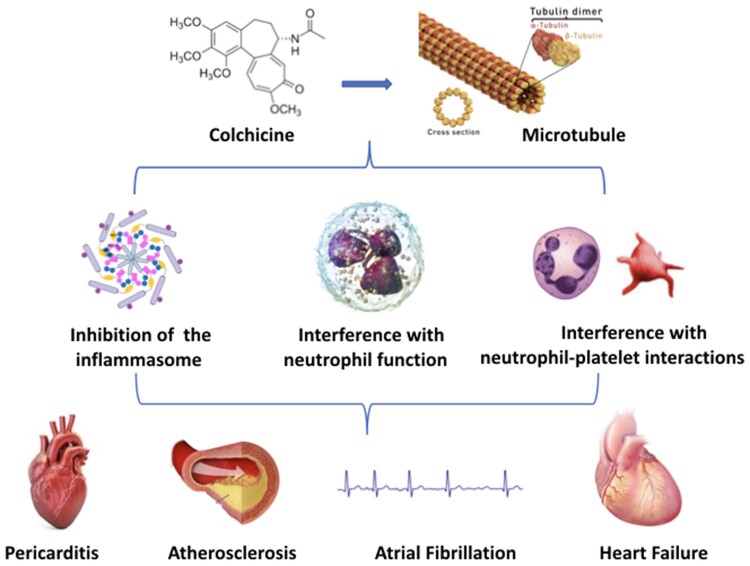
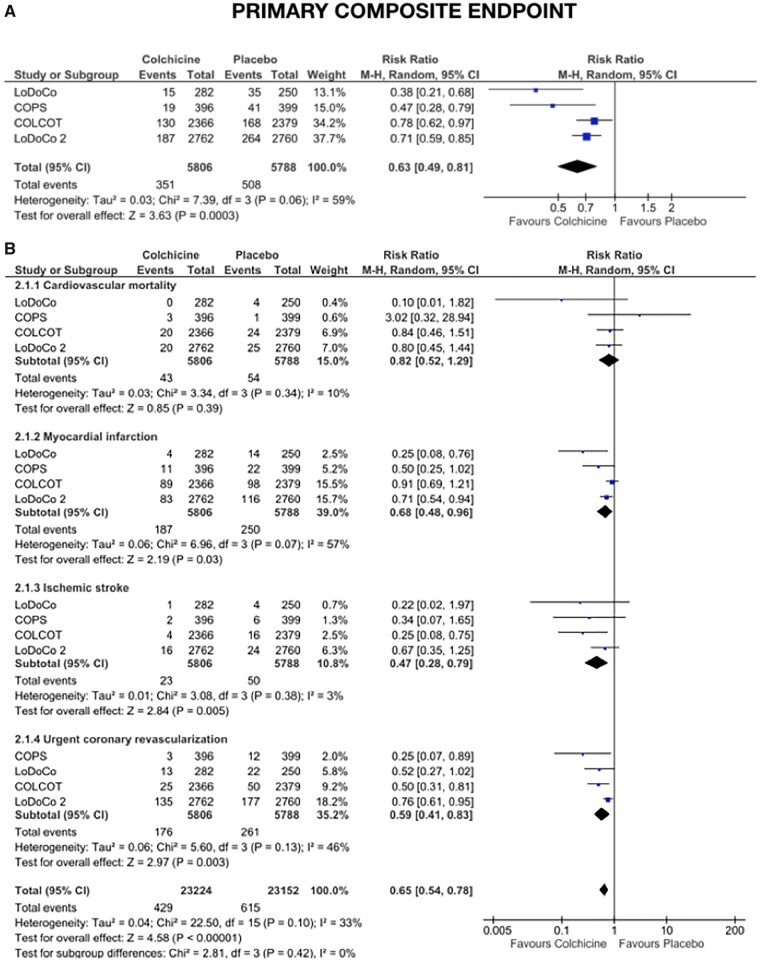
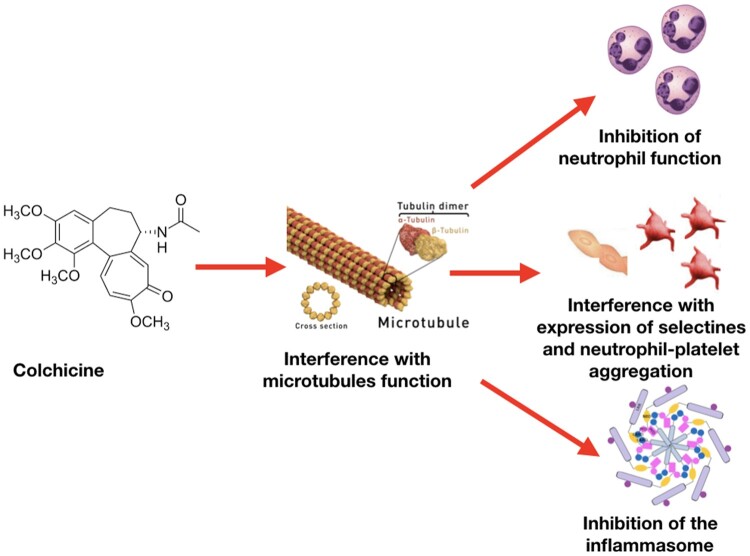
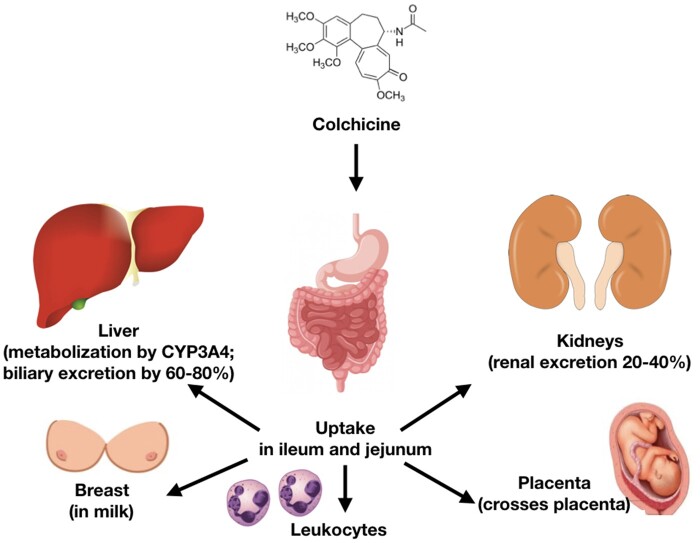
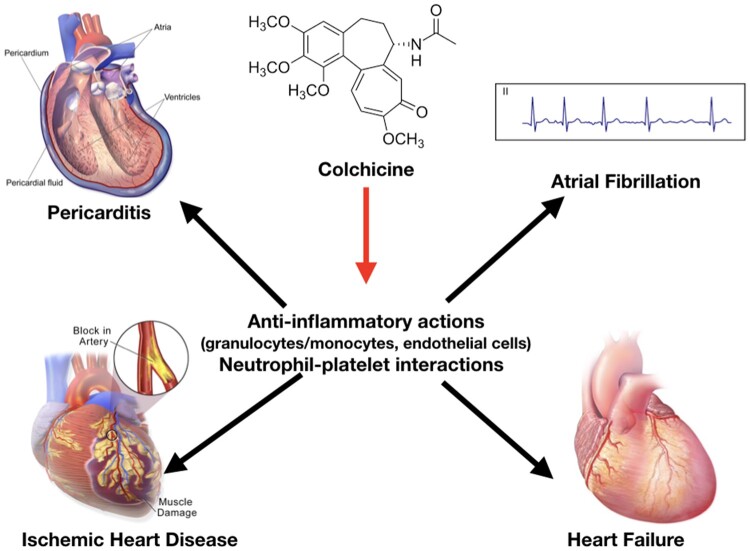
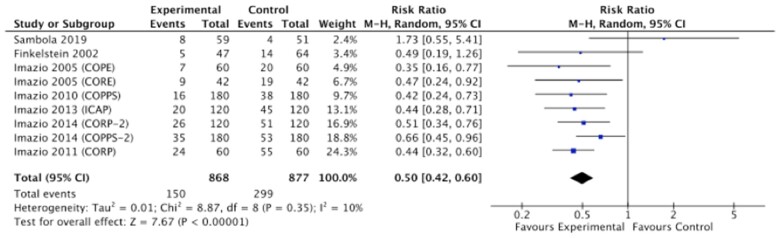
Colchicine is a unique, sophisticated anti-inflammatory agent that has been used for decades for the prevention of acute inflammatory flares in gout and familial Mediterranean fever. In recent years, clinical trials have demonstrated its potential in a range of cardiovascular (CV) conditions. Colchicine is avidly taken up by leucocytes, and its ability to bind to tubulin and interfere with microtubular function affects the expression of cytokines and interleukins, and the ability of neutrophils to marginate, ingress, aggregate, express superoxide, release neutrophil extracellular traps, and interact with platelets. In patients with acute and recurrent pericarditis, clinical trials in >1600 patients have consistently shown that colchicine halves the risk of recurrence [relative risk (RR) 0.50, 95% confidence interval (CI) 0.42-0.60]. In patients with acute and chronic coronary syndromes, multicentre randomized controlled trials in >11 000 patients followed for up to 5 years demonstrated that colchicine may reduce the risk of CV death, myocardial infarction, ischaemic stroke and ischaemia-driven revascularization by >30% (RR 0.63, 95% CI 0.49-0.81). The use of colchicine at doses of 0.5-1.0 mg daily in CV trials has proved safe. Early gastrointestinal intolerance limits its use in ∼10% of patients; however, ∼90% of patients tolerate it well over the long term. Despite isolated case reports, clinically relevant drug interactions with moderate to strong CYP3A4 inhibitors/competitors or P-glycoprotein inhibitors/competitors are rare if this dosage of colchicine is used in the absence of advanced renal or liver disease. The aim of this review is to summarize the contemporary data supporting the efficacy and safety of colchicine in patients with CV disease.
秋水仙碱是一种独特而复杂的抗炎药,已经使用了几十年,用于预防痛风和家族性地中海热的急性炎症发作。近年来,临床试验已经证明了它在一系列心血管(CV)疾病中的潜力。秋水仙碱被白细胞强烈摄取,其结合微管蛋白并干扰微管功能的能力会影响细胞因子和白细胞介素的表达,以及中性粒细胞边缘运动、进入、聚集、表达超氧化物、释放中性粒细胞胞外陷阱以及与血小板相互作用的能力。在急性和复发性心包炎患者中,超过 1600 名患者的临床试验一致表明,秋水仙碱可将复发风险降低一半[相对风险(RR)0.50,95%置信区间(CI)0.42-0.60]。在急性和慢性冠状动脉综合征患者中,超过 11000 名患者的多中心随机对照试验随访长达 5 年,表明秋水仙碱可能降低 30%以上的心血管死亡、心肌梗死、缺血性卒中和缺血驱动的血运重建风险(RR 0.63,95%CI 0.49-0.81)。在 CV 试验中,每天使用 0.5-1.0mg 的秋水仙碱剂量已被证明是安全的。早期胃肠道不耐受限制了其在约 10%患者中的使用;然而,超过 90%的患者在长期使用中耐受良好。尽管有个别病例报告,但如果在没有晚期肾脏或肝脏疾病的情况下使用这种剂量的秋水仙碱,与中度至强 CYP3A4 抑制剂/竞争物或 P-糖蛋白抑制剂/竞争物的临床相关药物相互作用很少见。本文旨在总结支持 CV 疾病患者使用秋水仙碱的有效性和安全性的当代数据。