Patel Trusharth, Watterson Christopher, McKenzie-Brown Anne Marie, Spektor Boris, Egan Katherine, Boorman David
Department of Anesthesiology, Division of Pain Management, Emory University School of Medicine, Atlanta, GA, 30308, USA.
Department of Radiology, Emory University School of Medicine, Atlanta, GA, 30308, USA.
J Pain Res. 2021 May 3;14:1193-1200. doi: 10.2147/JPR.S310238. eCollection 2021.
Radiofrequency ablation (RFA) is a denervation therapy commonly performed for pain of facet etiology. Degenerative spondylolisthesis, a malalignment of the spinal vertebrae, may be a co-existing condition contributing to pain; yet the effect of RFA on advancing listhesis is unknown. To the extent that denervating RFA may weaken paraspinal muscles that provide stability to the spine, the therapy can potentially contribute to progressive spinal instability.
Single-center, prospective, observational pilot study in an interventional pain practice to test the hypothesis that RFA of painful facets in the setting of spondylolisthesis may contribute to advancement of further degenerative spondylolisthesis. Fifteen participants with pre-existing degenerative Grade I or Grade II spondylolisthesis and coexisting axial lumbar pain underwent lumbar RFA encompassing spondylolisthesis level and followed with post-RFA imaging at 12 months and beyond to measure percent change in spondylolisthesis.
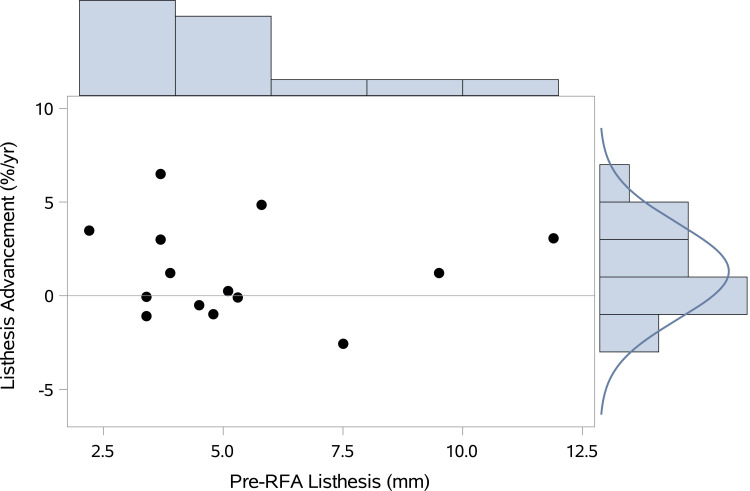
The primary outcome was the percent advancement of spondylolisthesis per year measured on post-RFA lateral lumbar spine imaging compared with non-intervention inferred baseline advancement of 2% per very limited observational studies. Among the 15 participants enrolled, 14 completed the study (median age 66; 64.3% women; median BMI 33.5; mean follow-up time 23.9 months). The mean advancement of spondylolisthesis per year after RFA was 1.30% (95% CI -0.14 to 2.78%), with 9/14 below 1.25%.
Among patients with lumbar pain originating from facets in the setting of degenerative spondylolisthesis who underwent lumbar RFA, the observed advancement of spondylolisthesis is clinically similar to the estimated maximum baseline of 2% per year change. The study findings did not find a destabilizing effect of lumbar RFA in advancing spondylolisthesis in this patient population.
射频消融术(RFA)是一种常用于治疗小关节源性疼痛的去神经疗法。退行性椎体滑脱,即脊椎的排列不齐,可能是导致疼痛的并存病症;然而,RFA对椎体滑脱进展的影响尚不清楚。由于去神经的RFA可能会削弱为脊柱提供稳定性的椎旁肌,该疗法可能会导致脊柱逐渐不稳定。
在一家介入疼痛诊所进行单中心、前瞻性、观察性试点研究,以检验以下假设:在椎体滑脱情况下对疼痛小关节进行RFA可能会导致进一步的退行性椎体滑脱进展。15名患有I级或II级退行性椎体滑脱且并存轴向腰痛的参与者接受了包括椎体滑脱节段的腰椎RFA,并在RFA后12个月及以后进行影像学检查,以测量椎体滑脱的百分比变化。
主要结局是根据RFA后腰椎侧位片测量的椎体滑脱每年进展百分比,与之相比,根据非常有限的观察性研究推断,非干预情况下的基线进展为每年2%。在纳入的15名参与者中,14名完成了研究(中位年龄66岁;64.3%为女性;中位BMI为33.5;平均随访时间23.9个月)。RFA后椎体滑脱每年的平均进展为1.30%(95%CI -0.14至2.78%),14名参与者中有9名低于1.25%。
在因退行性椎体滑脱导致腰痛且接受腰椎RFA的患者中,观察到的椎体滑脱进展在临床上与估计的每年2%变化的最大基线相似。该研究结果未发现腰椎RFA对该患者群体的椎体滑脱进展有不稳定作用。