Pituitary Clinic, Endocrinology Division, Department of Medicine, Hospital Universitario "Dr. José E. González" UANL, Monterrey, Mexico.
Neuroendocrinology Clinic, Department of Endocrinology and Metabolism, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico.
Front Endocrinol (Lausanne). 2021 Apr 26;12:657382. doi: 10.3389/fendo.2021.657382. eCollection 2021.
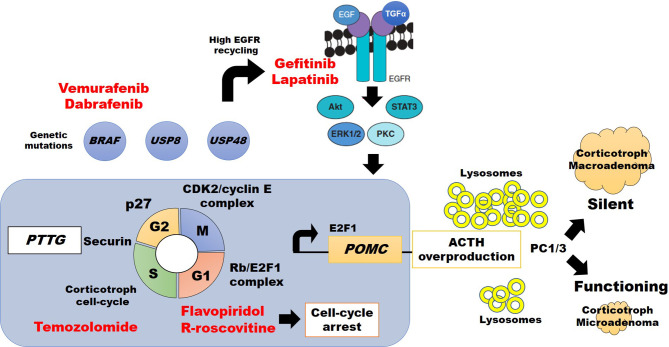
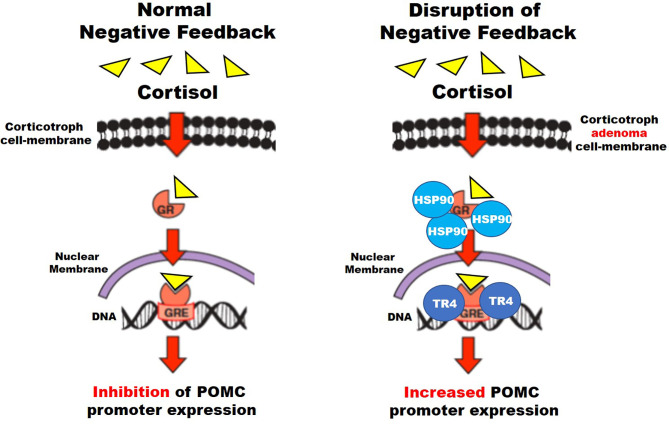
Corticotroph tumors (CTs) are pituitary neoplasms arising from the Tpit lineage, which may or not express adrenocorticotrophic hormone (ACTH). Functioning CTs cause Cushing's disease (CD), which has high morbidity and mortality due to hypercortisolemia. "Non-functioning" or silent CTs (SCT) and the Crooke's cell subtypes do not cause CD and may be asymptomatic until manifested by compressive symptoms and are more frequently found as macroadenoma. Both tend toward more aggressive behavior, recurrence, and a higher rate of malignant transformation to pituitary carcinoma. Tumorigenesis involves genetic, epigenetic, and post-transcriptional disruption of cell-cycle regulators, which increase cell proliferation, overexpression, ACTH transcription, and/or hypersecretion. Furthermore, functioning CTs develop resistance to glucocorticoid-mediated negative feedback on ACTH secretion, through increased expression of testicular orphan nuclear receptor 4 (TR4), heat-shock protein 90 (HSP90), and loss-of-function mutation of CDK5 and ABL enzyme substrate 1 () gene. Overt autonomous hypercortisolemia is difficult to control, and multiple diagnostic studies and therapeutic modalities are commonly required. Cell-cycle regulation depends mainly on p27, cyclin E, cyclin-dependent kinases (CDKs), and the retinoblastoma protein (Rb)/E2F1 transcription factor complex. Gain-of-function mutations of ubiquitin-specific protease () 8, , and genes may subsequently cause overexpression of epithelial growth factor receptor (EGFR), and enhance POMC transcription, cell proliferation, and tumor growth. Epigenetic changes through micro RNAs and decreased DNA deacetylation by histone deacetylase type 2 (HDAC2), may also affect tumor growth. All the former mechanisms may become interesting therapeutic targets for CTs, aside from temozolomide, currently used for aggressive tumors. Potential therapeutic agents are EGFR inhibitors such as gefitinib and lapatinib, the purine analog R-roscovitine by dissociation of CDK2/Cyclin E complex, the HSP90 inhibitor silibinin (novobiocin), to reduce resistance to glucocorticoid-mediated negative feedback, and BRAF inhibitors vemurafenib and dabrafenib in positive tumors. This review summarizes the molecular mechanisms related to CTs tumorigenesis, their diagnostic approach, and provides an update of the potential novel therapies, from the lab bench to the clinical translation.
促肾上腺皮质激素细胞瘤(CTs)是源自 Tpit 谱系的垂体肿瘤,可能表达或不表达促肾上腺皮质激素(ACTH)。功能性 CTs 导致库欣病(CD),由于皮质醇过多症,CD 的发病率和死亡率很高。“非功能性”或沉默 CT(SCT)和 Crooke 细胞亚型不引起 CD,可能无症状,直到表现为压迫症状,并且更常被发现为大腺瘤。两者都倾向于更具侵袭性的行为、复发和更高的恶性转化为垂体癌的发生率。肿瘤发生涉及细胞周期调节剂的遗传、表观遗传和转录后破坏,这会增加细胞增殖、过度表达、ACTH 转录和/或过度分泌。此外,功能性 CT 对 ACTH 分泌的糖皮质激素介导的负反馈产生抗性,这是通过增加睾丸孤儿核受体 4(TR4)、热休克蛋白 90(HSP90)和细胞周期蛋白依赖性激酶 5 和 ABL 酶底物 1 () 基因的失活突变来实现的。明显的自主高皮质醇血症难以控制,通常需要多种诊断研究和治疗方式。细胞周期调节主要取决于 p27、细胞周期蛋白 E、细胞周期蛋白依赖性激酶(CDKs)和视网膜母细胞瘤蛋白(Rb)/E2F1 转录因子复合物。泛素特异性蛋白酶 () 8、和基因的功能获得性突变可能随后导致表皮生长因子受体(EGFR)的过度表达,并增强 POMC 转录、细胞增殖和肿瘤生长。通过组蛋白去乙酰化酶 2(HDAC2)减少 DNA 去乙酰化和 microRNAs 的表观遗传变化也可能影响肿瘤生长。除了目前用于侵袭性肿瘤的替莫唑胺外,所有这些前机制都可能成为 CT 的有趣治疗靶点。潜在的治疗药物是 EGFR 抑制剂,如吉非替尼和拉帕替尼,嘌呤类似物 R-roscovitine 通过解离 CDK2/细胞周期蛋白 E 复合物,热休克蛋白 90 抑制剂水飞蓟素(诺维本),以降低对糖皮质激素介导的负反馈的抗性,以及 BRAF 抑制剂 vemurafenib 和 dabrafenib 在 BRAF 阳性肿瘤中。这篇综述总结了与 CT 肿瘤发生相关的分子机制,及其诊断方法,并提供了潜在的新疗法的最新进展,从实验室到临床转化。