Gámez-Díaz Laura, Seidel Markus G
Faculty of Medicine, Center for Chronic Immunodeficiency, Institute for Immunodeficiency, Medical Center, Albert-Ludwigs-University of Freiburg, Freiburg, Germany.
Division of Pediatric Hematology-Oncology, Department of Pediatrics and Adolescent Medicine, Medical University of Graz, Graz, Austria.
Front Pediatr. 2021 Apr 28;9:662645. doi: 10.3389/fped.2021.662645. eCollection 2021.
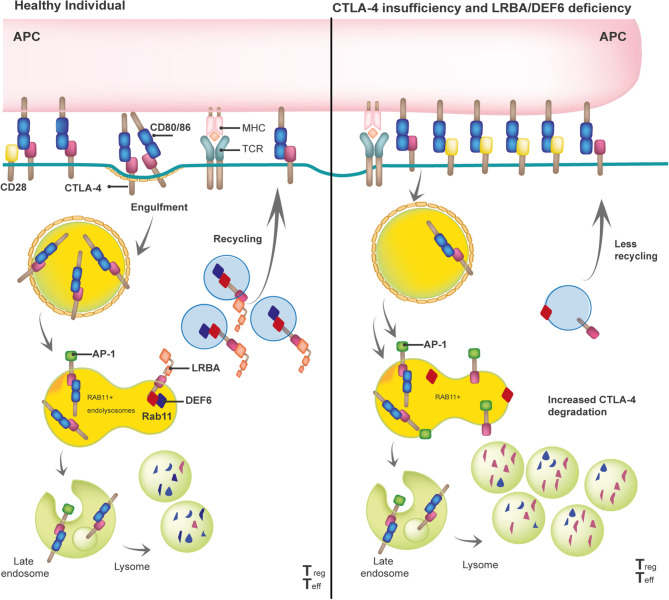
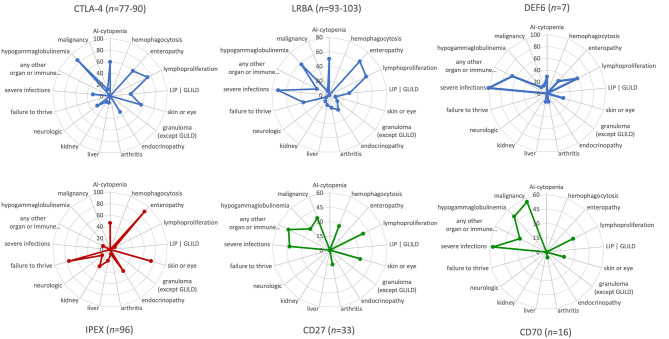
Cytotoxic T lymphocyte antigen-4 (CTLA-4) is a crucial immune checkpoint that is constitutively expressed in regulatory T (Treg) cells. Following T-cell activation, CTLA-4 is rapidly mobilized from its intracellular vesicle pool to the cell surface to control the availability of co-stimulatory B7 molecules, thereby maintaining immune homeostasis. Heterozygous mutations in lead to defects in (i) CTLA-4 ligand binding, (ii) homo-dimerization, (iii) B7-transendocytosis, and (iv) CTLA-4 vesicle trafficking, resulting in an inborn error of immunity with predominant autoimmunity. CTLA-4 vesicle trafficking impairment is also observed in patients with lipopolysaccharide-responsive beige-like anchor protein (LRBA) deficiency or the (DEF6) deficiency, caused by biallelic mutations in and , respectively. Therefore, patients with CTLA-4 insufficiency, LRBA deficiency, and-most recently reported-DEF6 deficiency present an overlapping clinical phenotype mainly attributed to a defective suppressive activity of Tregs, as all three diseases reduce overall surface expression of CTLA-4. In this paper, we describe the clinical phenotypes of these immune checkpoint defects, their patho-mechanisms, and visually compare them to other immune regulatory disorders (IPEX syndrome, CD27, and CD70 deficiencies) by using the immune deficiency and dysregulation (IDDA version 2.1) "kaleidoscope" score. This illustrates the variability of the degrees and manifestations of immune deficiency and dysregulation. Patients characteristically present with an increased risk of infections, autoimmune cytopenias, multi-organ autoimmunity, and inflammation, which are often severe and life-threatening. Furthermore, these patients suffer an increased risk of developing malignancies, especially Non-Hodgkin's lymphoma. Successful treatment options include regular administration of soluble CTLA-4-Ig fusion protein, Treg cell-sparing immune suppressants like sirolimus or mycophenolate mofetil, and hematopoietic stem cell transplantation. This mini-review highlights the most relevant biological and clinical features as well as treatment options for CTLA-4 insufficiency and LRBA and DEF6 deficiencies.
细胞毒性T淋巴细胞抗原4(CTLA-4)是一种关键的免疫检查点,在调节性T(Treg)细胞中组成性表达。T细胞激活后,CTLA-4迅速从其细胞内囊泡池转运至细胞表面,以控制共刺激B7分子的可用性,从而维持免疫稳态。CTLA-4基因杂合突变会导致以下缺陷:(i)CTLA-4配体结合;(ii)同源二聚化;(iii)B7转胞吞作用;(iv)CTLA-4囊泡运输,从而导致以自身免疫为主的先天性免疫缺陷。在脂多糖反应性米色样锚定蛋白(LRBA)缺陷或DEF6缺陷患者中也观察到CTLA-4囊泡运输受损,分别由LRBA基因和DEF6基因的双等位基因突变引起。因此,CTLA-4功能不全、LRBA缺陷以及最近报道的DEF6缺陷患者表现出重叠的临床表型,主要归因于Treg细胞抑制活性缺陷,因为这三种疾病都会降低CTLA-4的整体表面表达。在本文中,我们描述了这些免疫检查点缺陷的临床表型、其发病机制,并通过使用免疫缺陷和失调(IDDA版本2.1)“万花筒”评分,将它们与其他免疫调节障碍(IPEX综合征、CD27和CD70缺陷)进行直观比较。这说明了免疫缺陷和失调程度及表现的变异性。患者的特征是感染风险增加、自身免疫性血细胞减少、多器官自身免疫和炎症,这些情况往往严重且危及生命。此外,这些患者患恶性肿瘤的风险增加,尤其是非霍奇金淋巴瘤。成功的治疗选择包括定期给予可溶性CTLA-4-Ig融合蛋白、雷帕霉素或霉酚酸酯等保留Treg细胞的免疫抑制剂,以及造血干细胞移植。这篇综述强调了CTLA-4功能不全、LRBA和DEF6缺陷最相关的生物学和临床特征以及治疗选择。