Division of Pediatric Allergy and Immunology, Department of Pediatrics, Morsani College of Medicine, University of South Florida at Johns Hopkins All Children's Hospital, St Petersburg, FL, United States.
Department of Immunology, Hospital Clínico San Carlos, Instituto de Medicina del Laboratorio (IML), Complutense University of Madrid, Madrid, Spain.
Front Immunol. 2022 Jul 18;13:928062. doi: 10.3389/fimmu.2022.928062. eCollection 2022.
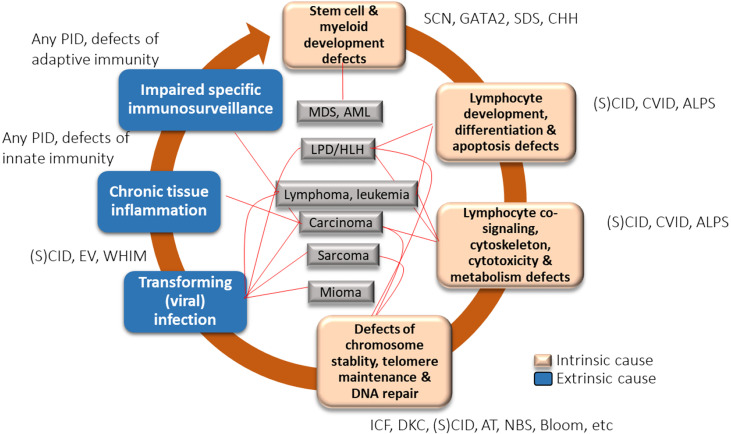
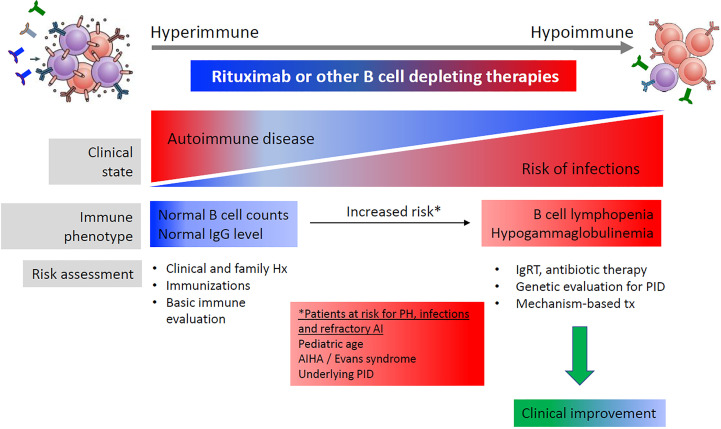
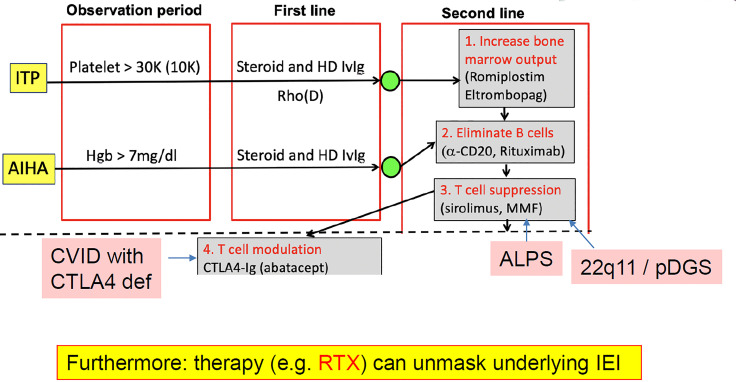
Primary immunodeficiencies (PIDs), a heterogenous group of inborn errors of immunity, are predetermined at birth but may evolve with age, leading to a variable clinical and laboratory presentation. In contrast, secondary immunodeficiencies (SIDs) are acquired declines of immune cell counts and or/function. The most common type of SID is a decreased antibody level occurring as a consequence of extrinsic influences, such as an underlying condition or a side effect of some medications used to treat hematological malignancies and autoimmune disorders. Paradoxically, immune deficiencies initially attributed to secondary causes may partly be due to an underlying PID. Therefore, in the era of immune-modulating biologicals, distinguishing between primary and secondary antibody deficiencies is of great importance. It can be difficult to unravel the relationship between PID, SID and hematological malignancy or autoimmunity in the clinical setting. This review explores SID and PID crossovers and discusses challenges to diagnosis and treatment strategies. The case of an immunodeficient patient with follicular lymphoma treated with rituximab illustrates how SID in the setting of hematological cancer can mask an underlying PID, and highlights the importance of screening such patients. The risk of hematological cancer is increased in PID: for example, lymphomas in PID may be driven by infections such as Epstein-Barr virus, and germline mutations associated with PID are enriched among patients with diffuse large B-cell lymphoma. Clues suggesting an increased risk of hematological malignancy in patients with common variable immune deficiency (CVID) are provided, as well as pointers for distinguishing PID versus SID in lymphoma patients. Two cases of patients with autoimmune disorders illustrate how an apparent rituximab-induced antibody deficiency can be connected to an underlying PID. We highlight that PID is increasingly recognized among patients with autoimmune cytopenias, and provide guidance on how to identify PID and distinguish it from SID in such patients. Overall, healthcare professionals encountering patients with malignancy and/or autoimmunity who have post-treatment complications of antibody deficiencies or other immune abnormalities need to be aware of the possibility of PID or SID and how to differentiate them.
原发性免疫缺陷病(PID)是一组先天免疫遗传错误,出生时即已确定,但可能随年龄而演变,导致临床表现和实验室检查结果多变。相比之下,继发性免疫缺陷病(SID)是免疫细胞数量和/或功能的获得性下降。SID 最常见的类型是由于外在影响(如潜在疾病或治疗血液恶性肿瘤和自身免疫性疾病的某些药物的副作用)导致的抗体水平下降。矛盾的是,最初归因于继发性原因的免疫缺陷部分可能是由于潜在的 PID。因此,在免疫调节生物制剂时代,区分原发性和继发性抗体缺陷非常重要。在临床环境中,要理清 PID、SID 和血液恶性肿瘤或自身免疫之间的关系可能颇具挑战。本文探讨了 SID 和 PID 的交叉点,并讨论了诊断和治疗策略所面临的挑战。一名滤泡性淋巴瘤伴免疫缺陷患者接受利妥昔单抗治疗的案例说明了血液恶性肿瘤背景下的 SID 如何掩盖潜在的 PID,并强调了对这类患者进行筛查的重要性。PID 患者发生血液恶性肿瘤的风险增加:例如,PID 中的淋巴瘤可能由感染(如 EBV)驱动,而与 PID 相关的种系突变在弥漫性大 B 细胞淋巴瘤患者中富集。本文还提供了提示普通变异性免疫缺陷(CVID)患者发生血液恶性肿瘤风险增加的线索,以及在淋巴瘤患者中区分 PID 与 SID 的要点。两名自身免疫性疾病患者的案例说明了看似由利妥昔单抗诱导的抗体缺陷如何与潜在的 PID 相关。我们强调 PID 在自身免疫性血细胞减少症患者中越来越常见,并提供了在这类患者中识别 PID 并将其与 SID 区分开来的指导。总之,遇到接受过治疗后出现抗体缺乏症或其他免疫异常并发症的伴有恶性肿瘤和/或自身免疫的患者的医疗保健专业人员,需要了解 PID 或 SID 的可能性,以及如何区分它们。