Department of Urology, Comprehensive Cancer Center, Medical University Vienna, Vienna General Hospital, Währinger Gürtel 18-20, 1090, Vienna, Austria.
Department of Urology, Medical University of Silesia, Zabrze, Poland.
World J Urol. 2021 Oct;39(10):3771-3779. doi: 10.1007/s00345-021-03715-4. Epub 2021 May 17.
To examine the predictive and prognostic value of preoperative Systemic Immune-inflammation Index (SII) in patients with radio-recurrent prostate cancer (PCa) treated with salvage radical prostatectomy (SRP).
This multicenter retrospective study included 214 patients with radio-recurrent PCa, treated with SRP between 2007 and 2015. SII was measured preoperatively (neutrophils × platelets/lymphocytes) and the cohort was stratified using optimal cut-off. Uni- and multivariable logistic and Cox regression analyses were performed to evaluate the predictive and prognostic value of SII as a preoperative biomarker.
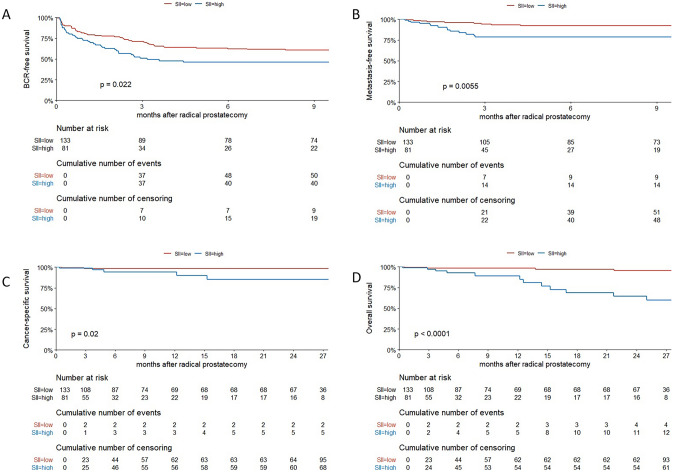
A total of 81 patients had high preoperative SII (≥ 730). On multivariable logistic regression modeling, high SII was predictive for lymph node metastases (OR 3.32, 95% CI 1.45-7.90, p = 0.005), and non-organ confined disease (OR 2.55, 95% CI 1.33-4.97, p = 0.005). In preoperative regression analysis, high preoperative SII was an independent prognostic factor for cancer-specific survival (CSS; HR 10.7, 95% CI 1.12-103, p = 0.039) and overall survival (OS; HR 8.57, 95% CI 2.70-27.2, p < 0.001). Similarly, in postoperative multivariable models, SII was associated with worse CSS (HR 22.11, 95% CI 1.23-398.12, p = 0.036) and OS (HR 5.98, 95% CI 1.67-21.44, p = 0.006). Notably, the addition of SII to preoperative reference models improved the C-index for the prognosis of CSS (89.5 vs. 80.5) and OS (85.1 vs 77.1).
In radio-recurrent PCa patients, high SII was associated with adverse pathological features at SRP and survival after SRP. Preoperative SII could help identify patients who might benefit from novel imaging modalities, multimodal therapy or a closer posttreatment surveillance.
探讨术前全身性免疫炎症指数(SII)在接受挽救性根治性前列腺切除术(SRP)治疗的放射性复发性前列腺癌(PCa)患者中的预测和预后价值。
本多中心回顾性研究纳入了 214 例 2007 年至 2015 年间接受 SRP 治疗的放射性复发性 PCa 患者。术前测量 SII(中性粒细胞×血小板/淋巴细胞),并使用最佳截断值对队列进行分层。采用单变量和多变量逻辑回归和 Cox 回归分析评估 SII 作为术前生物标志物的预测和预后价值。
共有 81 例患者术前 SII 较高(≥730)。多变量逻辑回归模型显示,高 SII 与淋巴结转移(OR 3.32,95%CI 1.45-7.90,p=0.005)和非器官局限性疾病(OR 2.55,95%CI 1.33-4.97,p=0.005)相关。在术前回归分析中,高术前 SII 是癌症特异性生存(CSS;HR 10.7,95%CI 1.12-103,p=0.039)和总生存(OS;HR 8.57,95%CI 2.70-27.2,p<0.001)的独立预后因素。同样,在术后多变量模型中,SII 与 CSS(HR 22.11,95%CI 1.23-398.12,p=0.036)和 OS(HR 5.98,95%CI 1.67-21.44,p<0.001)不良相关。值得注意的是,将 SII 加入术前参考模型可提高 CSS(89.5 vs. 80.5)和 OS(85.1 vs. 77.1)的预后 C 指数。
在放射性复发性 PCa 患者中,高 SII 与 SRP 时的不良病理特征和 SRP 后生存相关。术前 SII 可帮助识别可能受益于新型影像学方法、多模态治疗或更密切的治疗后监测的患者。