Rajwa Paweł, Życzkowski Marcin, Paradysz Andrzej, Slabon-Turska Monika, Suliga Kamil, Bujak Kamil, Bryniarski Piotr
Department of Urology, School of Medicine with the Division of Dentistry in Zabrze, Medical University of Silesia in Katowice, Zabrze, Poland.
3 Department of Cardiology, School of Medicine with the Division of Dentistry in Zabrze, Medical University of Silesia in Katowice, Silesian Center for Heart Diseases, Zabrze, Poland.
Arch Med Sci. 2017 Sep 21;16(5):1062-1071. doi: 10.5114/aoms.2017.70250. eCollection 2020.
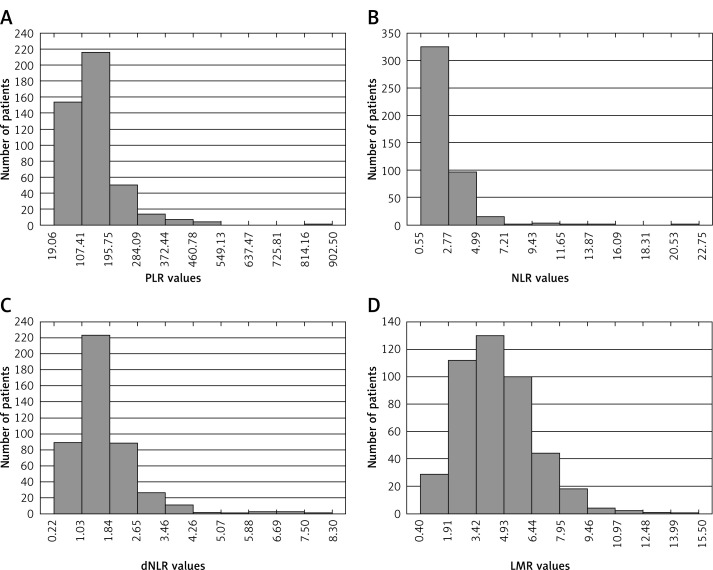
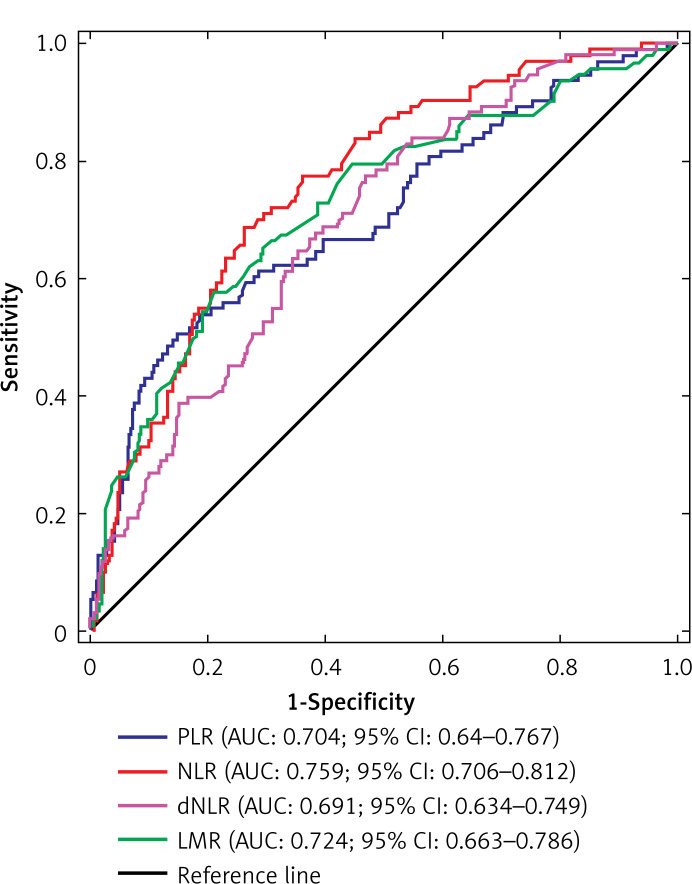
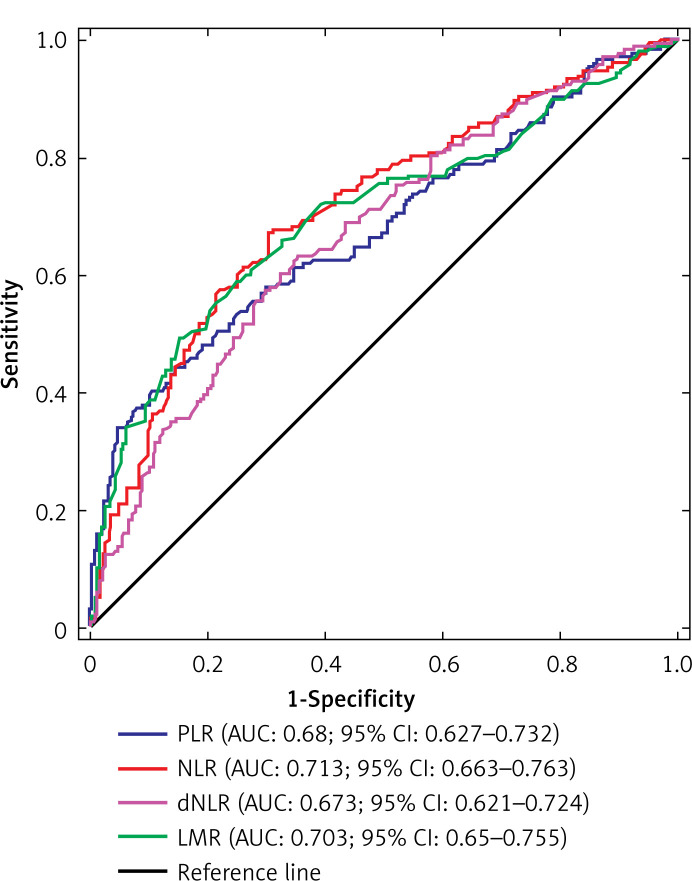
The association between novel blood-based inflammatory indices and patient survival has been reported with reference to various cancers. The aim of this study was to investigate the prognostic value of preoperative platelet-lymphocyte ratio (PLR), neutrophil-lymphocyte ratio (NLR), derived neutrophil-lymphocyte ratio (dNLR) and lymphocyte-monocyte ratio (LMR) in patients with renal cell carcinoma (RCC) treated with nephrectomy.
From 2003 to 2012, 455 patients who underwent partial or radical nephrectomy for RCC were enrolled in the study. The study endpoints were overall survival (OS) and cancer-specific survival (CSS).
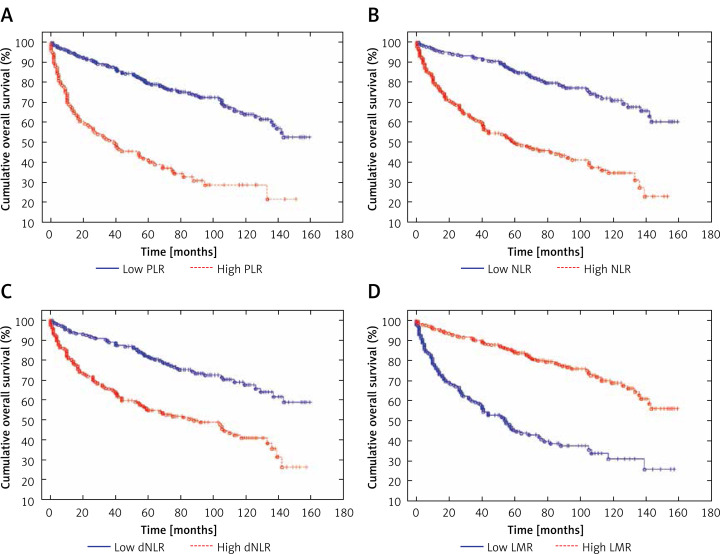
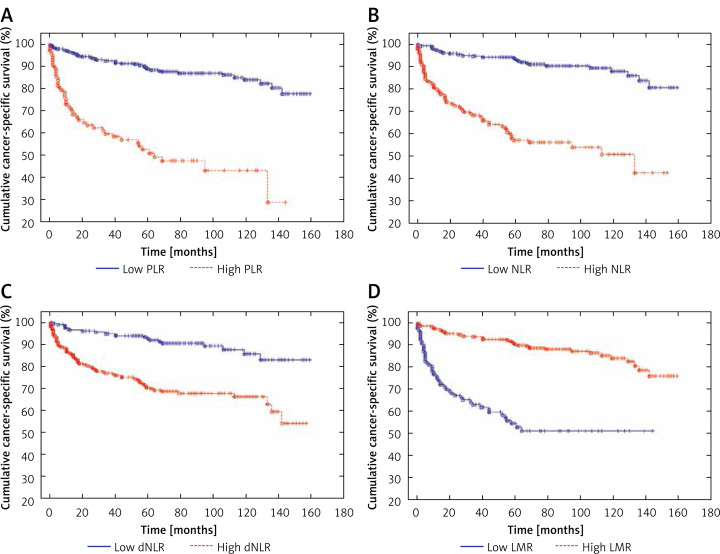
The median follow-up was 70 months. Groups of patients with high levels of PLR, NLR and dNLR and a low level of LMR more often underwent radical nephrectomy, had a higher cancer stage in the TNM classification, and were more frequently diagnosed with tumor necrosis in histopathological examination. Both cancer-specific mortality and overall mortality were significantly higher in patients with high PLR, NLR and dNLR and low LMR. Multivariate analysis of CSS, adjusted for standard clinicopathological factors, identified only dNLR ( = 0.006) as an independent prognostic factor. PLR ( = 0.0002), dNLR ( = 0.0003) and NLR ( = 0.002), but not LMR ( = 0.1), achieved prognostic significance in multivariable analysis regarding OS.
Only dNLR was an independent prognostic factor for CSS and OS. Nevertheless, our study indicates that all examined complete blood count-based biomarkers may be useful tools in managing RCC patients treated with a surgical approach.
关于各种癌症,已有报道新型血液炎症指标与患者生存率之间的关联。本研究旨在探讨术前血小板淋巴细胞比值(PLR)、中性粒细胞淋巴细胞比值(NLR)、衍生中性粒细胞淋巴细胞比值(dNLR)和淋巴细胞单核细胞比值(LMR)在接受肾切除术治疗的肾细胞癌(RCC)患者中的预后价值。
2003年至2012年,455例因RCC接受部分或根治性肾切除术的患者纳入本研究。研究终点为总生存期(OS)和癌症特异性生存期(CSS)。
中位随访时间为70个月。PLR、NLR和dNLR水平高且LMR水平低的患者组更常接受根治性肾切除术,在TNM分类中癌症分期更高,在组织病理学检查中更常被诊断为肿瘤坏死。PLR、NLR和dNLR水平高且LMR水平低的患者的癌症特异性死亡率和总死亡率均显著更高。对CSS进行多变量分析,并根据标准临床病理因素进行调整,仅dNLR(P = 0.006)被确定为独立预后因素。在关于OS的多变量分析中,PLR(P = 0.0002)、dNLR(P = 0.0003)和NLR(P = 0.002)具有预后意义,但LMR(P = 0.1)无此意义。
仅dNLR是CSS和OS的独立预后因素。然而,我们的研究表明,所有检测的基于全血细胞计数的生物标志物可能是管理接受手术治疗的RCC患者的有用工具。