Centre for the Study of Regional Development, School of Social Sciences, Jawaharlal Nehru University, New Delhi, India.
BMC Public Health. 2021 May 17;21(1):939. doi: 10.1186/s12889-021-10773-1.
Population aging poses a demographic burden on a country such as India with inadequate social security systems and very low public investment in health sector. This challenge of accelerated demographic transition is coupled by the rural-urban disparity in access to healthcare services among the elderly people in India. An important objective of India's National Health Policy (2017) is to "progressively achieve universal health coverage" which is posited upon mitigating the sub-national disparity that necessitates identifying the drivers of the disparity for targeted policy intervention. This study, therefore, makes an attempt towards the exploration of the prominent contributory factors behind the rural-urban gap in utilisation of healthcare among the older population in India.
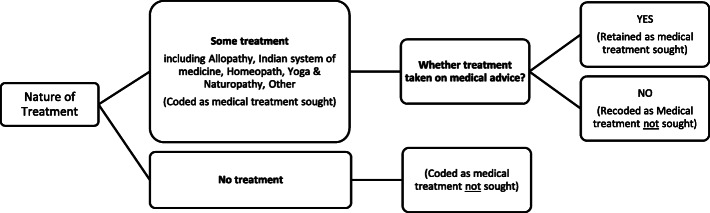
The analysis has been done by using the unit level data of Social Consumption: Health (Schedule number 25.0) of the 75th round of the National sample Survey conducted during July 2017-June 2018. Two binary logistic models have been proposed to capture the crude and the adjusted association between health seeking behaviour and place of residence (rural/ urban). To compute the group differences (between rural and urban) in the rate of healthcare utilization among the elderly population in India and to decompose these differences into the major contributing factors, Fairlie's decomposition method has been employed.
The logistic regression models established a strong association between place of residence and likelihood of healthcare utilisation among the Indian elderly people. The results of the Fairlie's decomposition analysis revealed considerable rural-urban inequality disfavouring the rural residents and health care utilisation was found to be 7 percentage points higher among the older population residing in urban India than their rural counterparts. Level of education and economic status, both of which are indicators of a person's Socio-Economic Status, were the two major determinants of the existing rural-urban differential in healthcare utilisation, together explaining 41% of the existing rural-urban differential.
Public health care provisions need to be strengthened both in terms of quality and outreach by way of greater public investments in the health sector and by building advanced health infrastructure in the rural areas. Implementation of poverty alleviation programmes and ensuring social-security of the elderly are also indispensable in bringing about equity in healthcare utilisation.
人口老龄化给印度这样的社会保障体系不足、公共卫生部门投资极低的国家带来了人口负担。印度老年人在获得医疗保健服务方面存在城乡差距,这一挑战与人口快速转变相叠加。印度 2017 年国家卫生政策的一个重要目标是“逐步实现全民健康覆盖”,这需要减轻国家内部的差距,这就需要确定造成这种差距的驱动因素,以便有针对性地采取政策干预措施。因此,本研究试图探索印度老年人城乡医疗保健利用差距背后的主要促成因素。
本分析使用了 2017 年 7 月至 2018 年 6 月期间进行的第 75 轮全国抽样调查的社会消费:健康(附表 25.0)的单位级数据。提出了两个二项逻辑模型,以捕捉卫生保健寻求行为与居住地(农村/城市)之间的原始和调整关联。为了计算印度老年人口中城乡之间医疗保健利用率的差异(城乡之间),并将这些差异分解为主要促成因素,采用了费尔利分解方法。
逻辑回归模型建立了居住地与印度老年人卫生保健利用之间的强关联。费尔利分解分析的结果显示,城乡之间存在相当大的不平等,不利于农村居民,居住在印度城市的老年人的医疗保健利用率比农村同龄人高 7 个百分点。教育水平和经济地位都是一个人社会经济地位的指标,是造成现有城乡医疗保健利用差异的两个主要决定因素,共同解释了现有城乡差异的 41%。
需要通过增加对卫生部门的公共投资和在农村地区建设先进的卫生基础设施,在质量和覆盖面两方面加强公共医疗保健服务。实施扶贫计划和确保老年人的社会保障也是实现医疗保健利用公平的不可或缺的因素。