Centre for Heart Rhythm Disorders, The University of Adelaide, Adelaide, Australia.
Flinders University, Adelaide, Australia.
JMIR Mhealth Uhealth. 2021 May 19;9(5):e24470. doi: 10.2196/24470.
Atrial fibrillation (AF) screening using mobile single-lead electrocardiogram (ECG) devices has demonstrated variable sensitivity and specificity. However, limited data exists on the use of such devices in low-resource countries.
The goal of the research was to evaluate the utility of the KardiaMobile device's (AliveCor Inc) automated algorithm for AF screening in a semirural Ethiopian population.
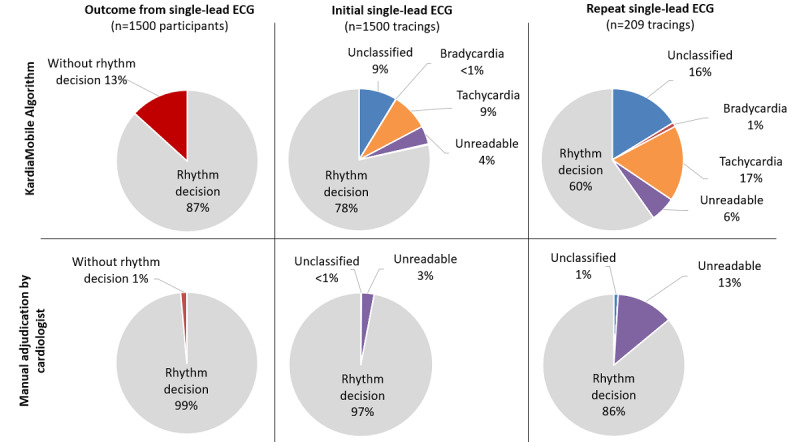
Analysis was performed on 30-second single-lead ECG tracings obtained using the KardiaMobile device from 1500 TEFF-AF (The Heart of Ethiopia: Focus on Atrial Fibrillation) study participants. We evaluated the performance of the KardiaMobile automated algorithm against cardiologists' interpretations of 30-second single-lead ECG for AF screening.
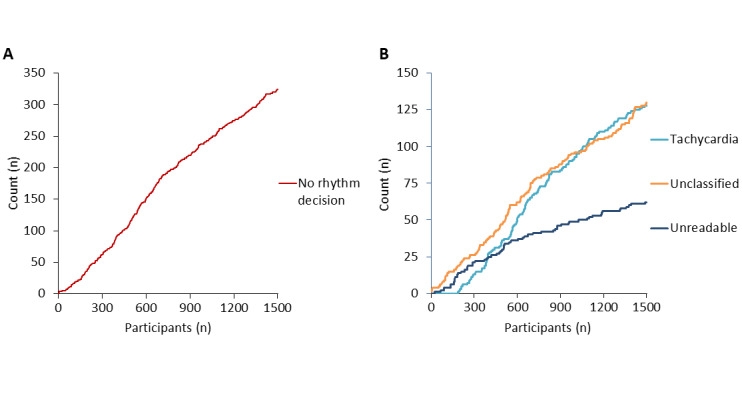
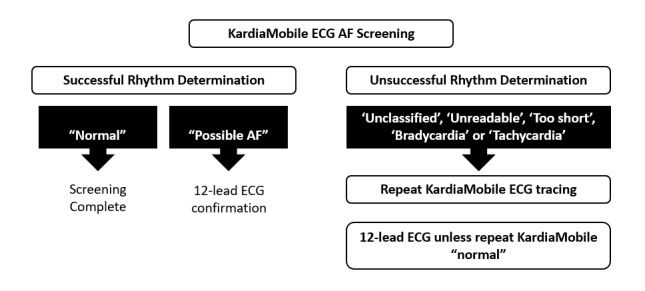
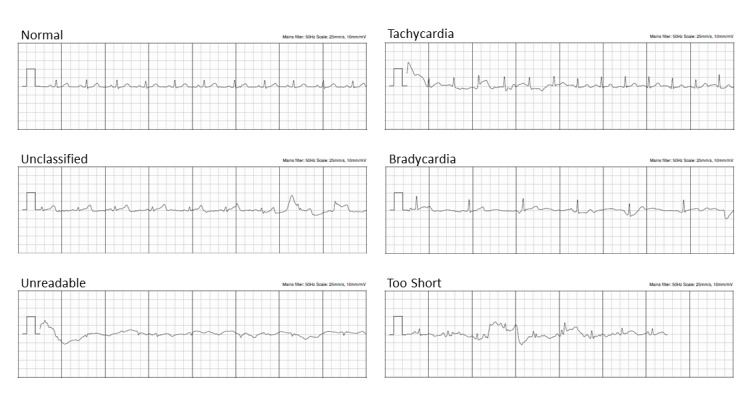
A total of 1709 single-lead ECG tracings (including repeat tracing on 209 occasions) were analyzed from 1500 Ethiopians (63.53% [953/1500] male, mean age 35 [SD 13] years) who presented for AF screening. Initial successful rhythm decision (normal or possible AF) with one single-lead ECG tracing was lower with the KardiaMobile automated algorithm versus manual verification by cardiologists (1176/1500, 78.40%, vs 1455/1500, 97.00%; P<.001). Repeat single-lead ECG tracings in 209 individuals improved overall rhythm decision, but the KardiaMobile automated algorithm remained inferior (1301/1500, 86.73%, vs 1479/1500, 98.60%; P<.001). The key reasons underlying unsuccessful KardiaMobile automated rhythm determination include poor quality/noisy tracings (214/408, 52.45%), frequent ectopy (22/408, 5.39%), and tachycardia (>100 bpm; 167/408, 40.93%). The sensitivity and specificity of rhythm decision using KardiaMobile automated algorithm were 80.27% (1168/1455) and 82.22% (37/45), respectively.
The performance of the KardiaMobile automated algorithm was suboptimal when used for AF screening. However, the KardiaMobile single-lead ECG device remains an excellent AF screening tool with appropriate clinician input and repeat tracing.
Australian New Zealand Clinical Trials Registry ACTRN12619001107112; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=378057&isReview=true.
使用移动单导联心电图(ECG)设备进行心房颤动(AF)筛查的敏感性和特异性存在差异。然而,在资源有限的国家中,此类设备的使用数据有限。
本研究旨在评估 KardiaMobile 设备(AliveCor Inc)的自动算法在埃塞俄比亚半农村地区人群中用于 AF 筛查的效用。
对 TEFF-AF(埃塞俄比亚之心:关注心房颤动)研究的 1500 名参与者使用 KardiaMobile 设备获得的 30 秒单导联 ECG 描记进行分析。我们评估了 KardiaMobile 自动算法对 KardiaMobile 自动算法对 30 秒单导联 ECG 进行 AF 筛查的cardiologists 解释的性能。
从 1500 名接受 AF 筛查的埃塞俄比亚人(63.53%[953/1500]男性,平均年龄 35[SD 13]岁)中分析了总共 1709 个单导联 ECG 描记(包括 209 次重复描记)。使用 KardiaMobile 自动算法与 cardiologists 手动验证相比,单次单导联 ECG 描记的初始成功节律判断(正常或可能的 AF)较低(1176/1500,78.40%,vs 1455/1500,97.00%;P<.001)。在 209 名个体中重复单导联 ECG 描记改善了整体节律判断,但 KardiaMobile 自动算法仍较差(1301/1500,86.73%,vs 1479/1500,98.60%;P<.001)。导致 KardiaMobile 自动节律确定不成功的主要原因包括质量差/嘈杂的描记(214/408,52.45%)、频繁的异位(22/408,5.39%)和心动过速(>100 bpm;167/408,40.93%)。使用 KardiaMobile 自动算法进行节律判断的灵敏度和特异性分别为 80.27%(1168/1455)和 82.22%(37/45)。
当用于 AF 筛查时,KardiaMobile 自动算法的性能不理想。然而,KardiaMobile 单导联 ECG 设备仍然是一种出色的 AF 筛查工具,可通过适当的临床医生输入和重复描记进行使用。
澳大利亚和新西兰临床试验注册 ACTRN12619001107112;https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=378057&isReview=true。