Department of Experimental and Clinical Medicine, University of Catanzaro, Catanzaro, Italy.
Department of Medical and Surgical Sciences, University of Catanzaro, Catanzaro, Italy.
PLoS One. 2021 May 21;16(5):e0252209. doi: 10.1371/journal.pone.0252209. eCollection 2021.
Acute Kidney Injury (AKI) represents a clinical condition with poor prognosis. The incidence of AKI in hospitalized patients was about 22-57%. Patients undergoing cardiac surgery (CS) are particularly exposed to AKI because of the related oxidative stress, inflammation and ischemia-reperfusion damage. Hence, the risk profile of patients undergoing CS who develop AKI and who are consequently at increased mortality risk deserves further investigation.
We designed a retrospective study examining consecutive patients undergoing any type of open-heart surgery from January to December 2018. Patients with a history of AKI were excluded. AKI was diagnosed according to KDIGO criteria. Univariate associations between clinical variables and AKI were tested using logistic regression analysis. Variable thresholds maximizing the association with AKI were measured with the Youden index. Multivariable logistic regression analysis was performed to assess predictors of AKI through backward selection. Mortality risk factors were assessed through the Cox proportional hazard model.
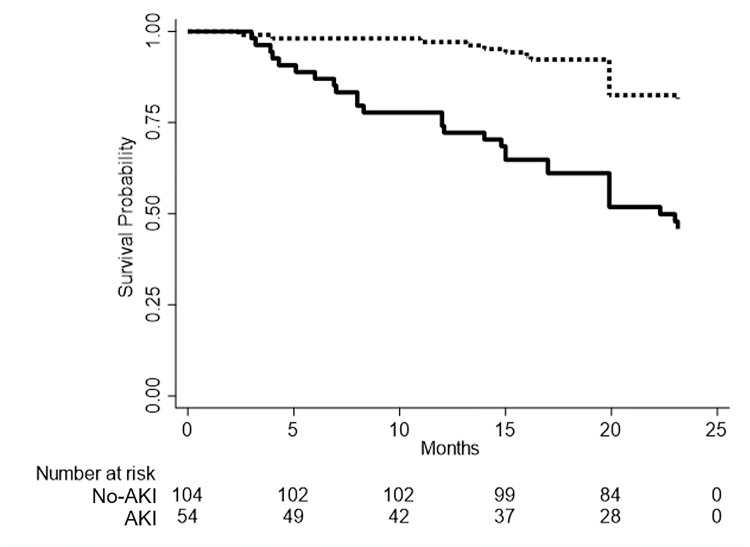
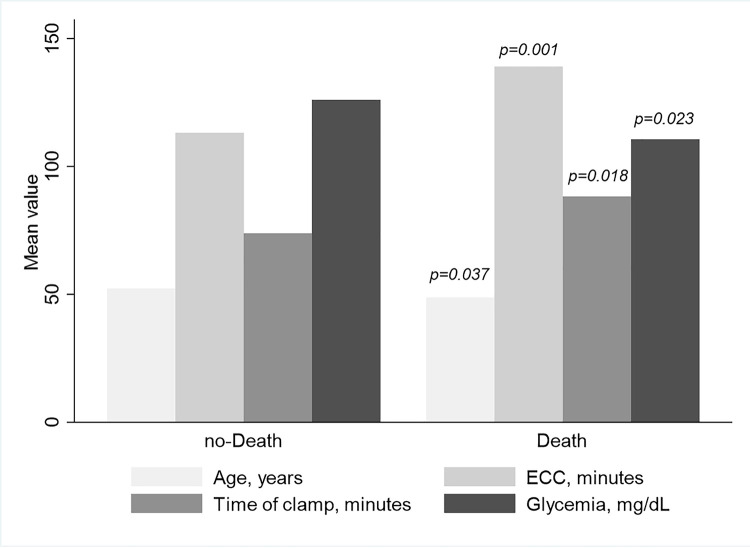
We studied 158 patients (mean age 51.2±9.7 years) of which 74.7% were males. Types of procedures performed were: isolated coronary artery bypass (CABG, 50.6%), valve (28.5%), aortic (3.2%) and combined (17.7%) surgery. Overall, incidence of AKI was 34.2%. At multivariable analysis, young age (p = 0.016), low blood glucose levels (p = 0.028), estimated Glomerular Filtration Rate (p = 0.007), pH (p = 0.008), type of intervention (p = 0.031), prolonged extracorporeal circulation (ECC, p = 0.028) and cross-clamp (p = 0.021) times were associated with AKI. The threshold for detecting AKI were 91 and 51 minutes for ECC and cross-clamp times, respectively. At survival analysis, the presence of AKI, prolonged ECC and cross-clamp times, and low blood glucose levels forecasted mortality.
AKI is common among CS patients and associates with shortened life-expectancy. Several pre-operative and intra-operative predictors are associated with AKI and future mortality. Future studies, aiming at improving prognosis in high-risk patients, by a stricter control of these factors, are awaited.
急性肾损伤(AKI)是一种预后不良的临床病症。住院患者 AKI 的发病率约为 22-57%。由于相关的氧化应激、炎症和缺血再灌注损伤,接受心脏手术(CS)的患者尤其容易发生 AKI。因此,需要进一步研究发生 AKI 的 CS 患者的风险状况,以及这些患者因 AKI 导致死亡率升高的原因。
我们设计了一项回顾性研究,纳入了 2018 年 1 月至 12 月期间接受任何类型的体外循环心脏手术的连续患者。排除有 AKI 病史的患者。AKI 的诊断依据 KDIGO 标准。使用逻辑回归分析测试临床变量与 AKI 之间的单变量关联。使用约登指数测量与 AKI 关联最大的变量阈值。通过向后选择进行多变量逻辑回归分析,以评估 AKI 的预测因素。通过 Cox 比例风险模型评估死亡率的危险因素。
我们研究了 158 名患者(平均年龄 51.2±9.7 岁),其中 74.7%为男性。进行的手术类型包括:单纯冠状动脉旁路移植术(CABG,50.6%)、瓣膜(28.5%)、主动脉(3.2%)和联合(17.7%)手术。总体而言,AKI 的发生率为 34.2%。多变量分析显示,年龄较小(p=0.016)、血糖水平较低(p=0.028)、估计肾小球滤过率(p=0.007)、pH 值(p=0.008)、手术类型(p=0.031)、体外循环时间延长(p=0.028)和主动脉阻断时间延长(p=0.021)与 AKI 相关。ECC 和主动脉阻断时间的 AKI 检测阈值分别为 91 分钟和 51 分钟。在生存分析中,AKI 的存在、ECC 和主动脉阻断时间延长以及血糖水平较低预测了死亡率。
AKI 在 CS 患者中很常见,并与预期寿命缩短有关。一些术前和术中的预测因素与 AKI 和未来的死亡率相关。期待未来的研究通过更严格地控制这些因素,来改善高危患者的预后。