Department of Medical Statistics, LSHTM, Keppel Street, London, WC1E 7HT, UK.
Clinical Trials Unit, LSHTM, Keppel Street, London, WC1E 7HT, UK.
Trials. 2021 May 22;22(1):357. doi: 10.1186/s13063-021-05266-w.
In large multicentre trials in diverse settings, there is uncertainty about the need to adjust for centre variation in design and analysis. A key distinction is the difference between variation in outcome (independent of treatment) and variation in treatment effect. Through re-analysis of the CRASH-2 trial (2010), this study clarifies when and how to use multi-level models for multicentre studies with binary outcomes.
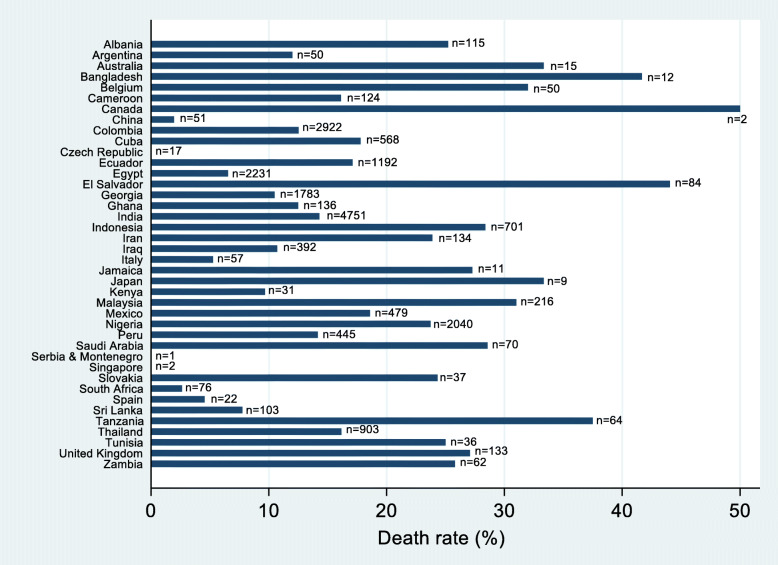
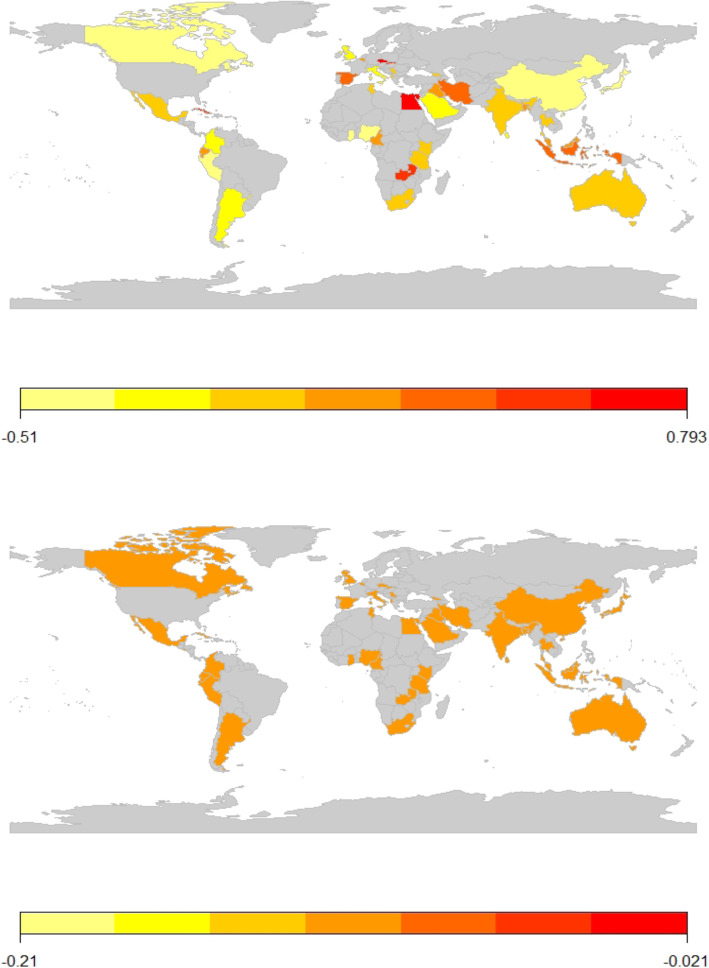
CRASH-2 randomised 20,127 trauma patients across 271 centres and 40 countries to either single-dose tranexamic acid or identical placebo, with all-cause death at 4 weeks the primary outcome. The trial data had a hierarchical structure, with patients nested in hospitals which in turn are nested within countries. Reanalysis of CRASH-2 trial data assessed treatment effect and both patient and centre level baseline covariates as fixed effects in logistic regression models. Random effects were included to assess where there was variation between countries, and between centres within countries, both in underlying risk of death and in treatment effect.
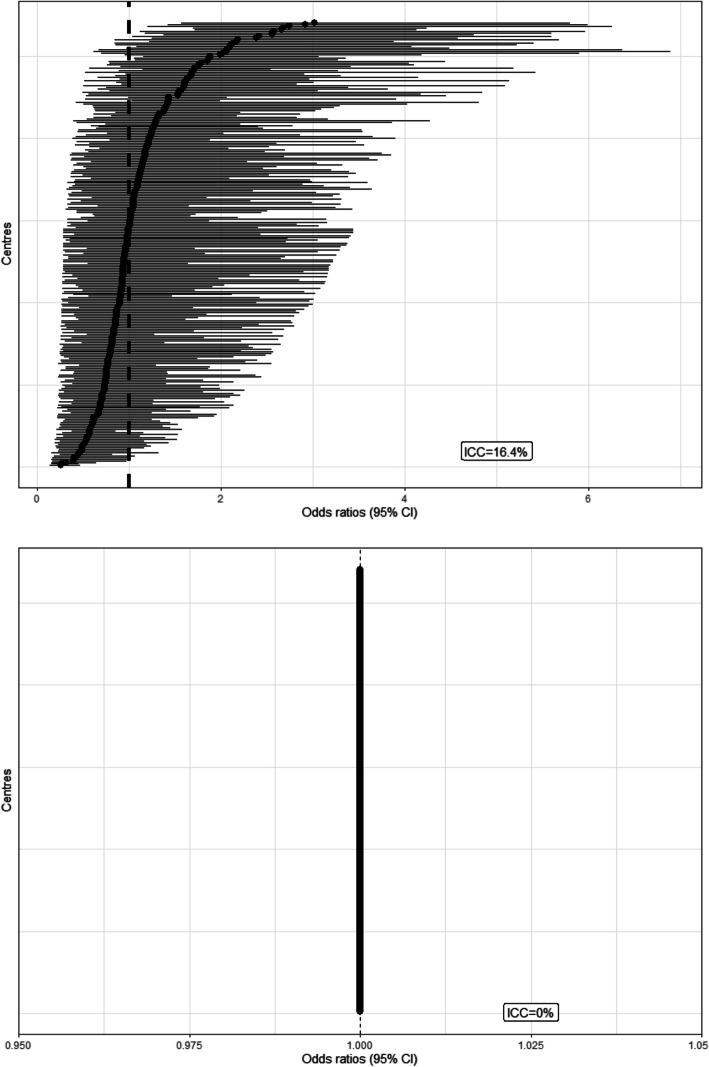
In CRASH-2, there was significant variation between countries and between centres in death at 4 weeks, but absolutely no differences between countries or centres in the effect of treatment. Average treatment effect was not altered after accounting for centre and country variation in this study.
It is important to distinguish between underlying variation in outcomes and variation in treatment effects; the former is common but the latter is not. Stratifying randomisation by centre overcomes many statistical problems and including random intercepts in analysis may increase power and decrease bias in mean and standard error estimates.
Current Controlled Trials ISRCTN86750102 , ClinicalTrials.gov NCT00375258 , and South African Clinical Trial Register DOH-27-0607-1919.
在不同环境下的大型多中心试验中,对于在设计和分析中是否需要调整中心变异存在不确定性。一个关键区别是结局(独立于治疗)的变异性与治疗效果的变异性之间的差异。通过对 CRASH-2 试验(2010 年)的重新分析,本研究阐明了何时以及如何使用多水平模型来分析具有二分类结局的多中心研究。
CRASH-2 试验将 20127 名创伤患者随机分配至 271 个中心和 40 个国家,分别接受单次剂量氨甲环酸或相同的安慰剂治疗,以 4 周时的全因死亡率为主要结局。该试验数据具有层次结构,患者嵌套于医院,医院又嵌套于国家。对 CRASH-2 试验数据的重新分析评估了治疗效果以及患者和中心水平的基线协变量作为逻辑回归模型中的固定效应。随机效应用于评估国家之间以及国家内的中心之间在死亡的潜在风险和治疗效果方面的差异。
在 CRASH-2 试验中,4 周时的死亡率在国家和中心之间存在显著差异,但在国家和中心之间,治疗效果没有差异。在本研究中,考虑到中心和国家变异后,平均治疗效果没有改变。
区分结局的潜在变异性和治疗效果的变异性非常重要;前者很常见,但后者并非如此。通过中心分层随机化可以解决许多统计学问题,并且在分析中包含随机截距可能会增加平均和标准误估计的功效并减少偏差。
当前对照试验 ISRCTN86750102,ClinicalTrials.gov NCT00375258,南非临床试验注册 DOH-27-0607-1919。