Department of Obstetrics, Gynecology and Reproductive Sciences, Magee-Womens Research Institute, University of Pittsburgh, Pittsburgh, PA, USA.
Department of Health Policy and Management, University of Pittsburgh, Pittsburgh, PA, USA.
Addiction. 2021 Dec;116(12):3504-3514. doi: 10.1111/add.15582. Epub 2021 Jun 9.
To test the effect of the duration of medication for opioid use disorder (MOUD) use during pregnancy on maternal, perinatal and neonatal outcomes.
Retrospective cohort analysis of claims, encounter and pharmacy data.
Pennsylvania, USA.
We analyzed 13 320 pregnancies among 10 741 women with opioid use disorder aged 15-44 years enrolled in Pennsylvania Medicaid between 2009 and 2017.
We examined five outcomes during pregnancy and for 12 weeks postpartum: (1) overdose, (2) postpartum MOUD continuation, (3) preterm birth (< 37 weeks gestation), (4) term low birth weight (< 2500 g at ≥ 37 weeks) and (5) neonatal abstinence syndrome (NAS). Our primary exposure was the duration (count of weeks) of any MOUD use, including methadone or buprenorphine, during pregnancy.
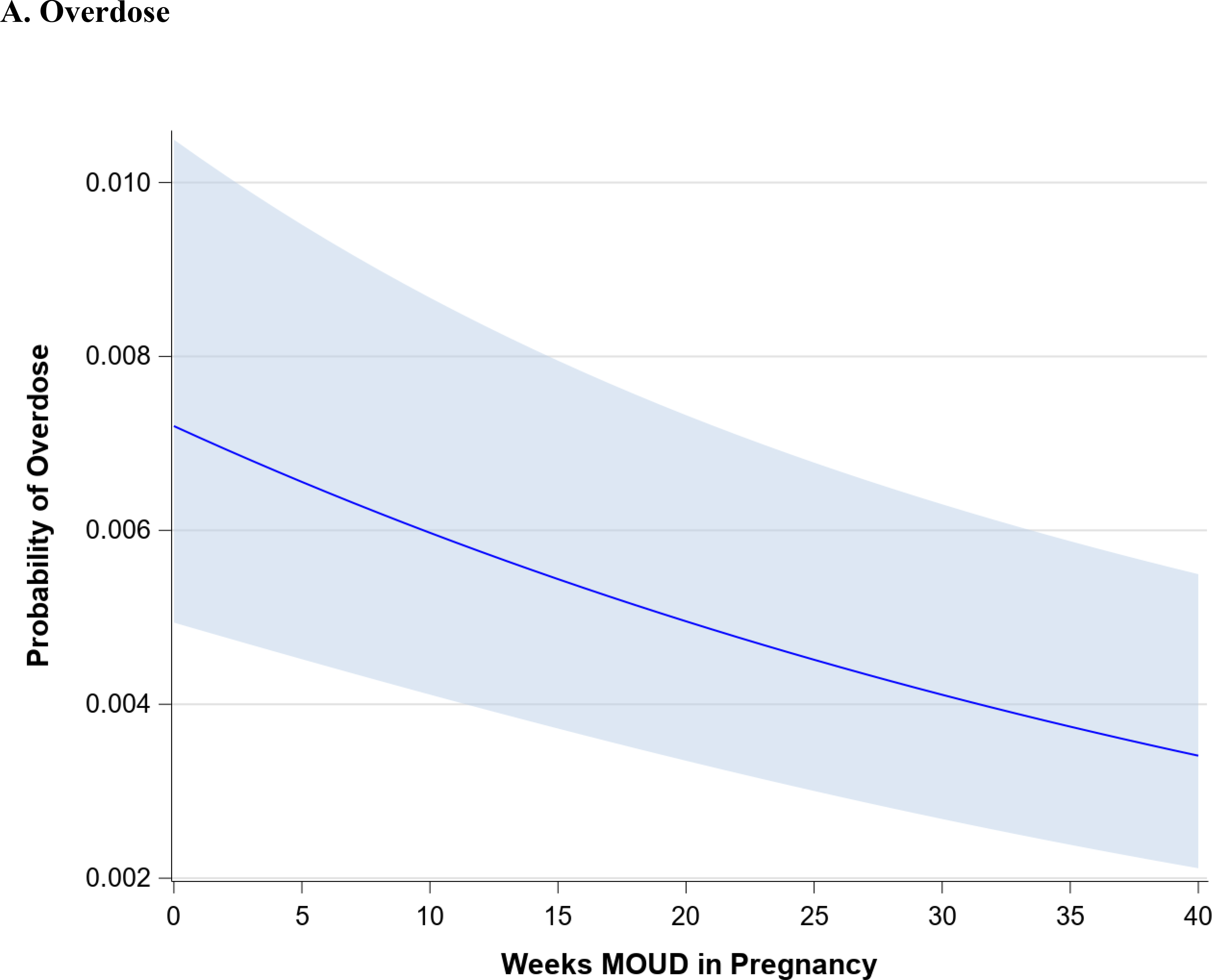
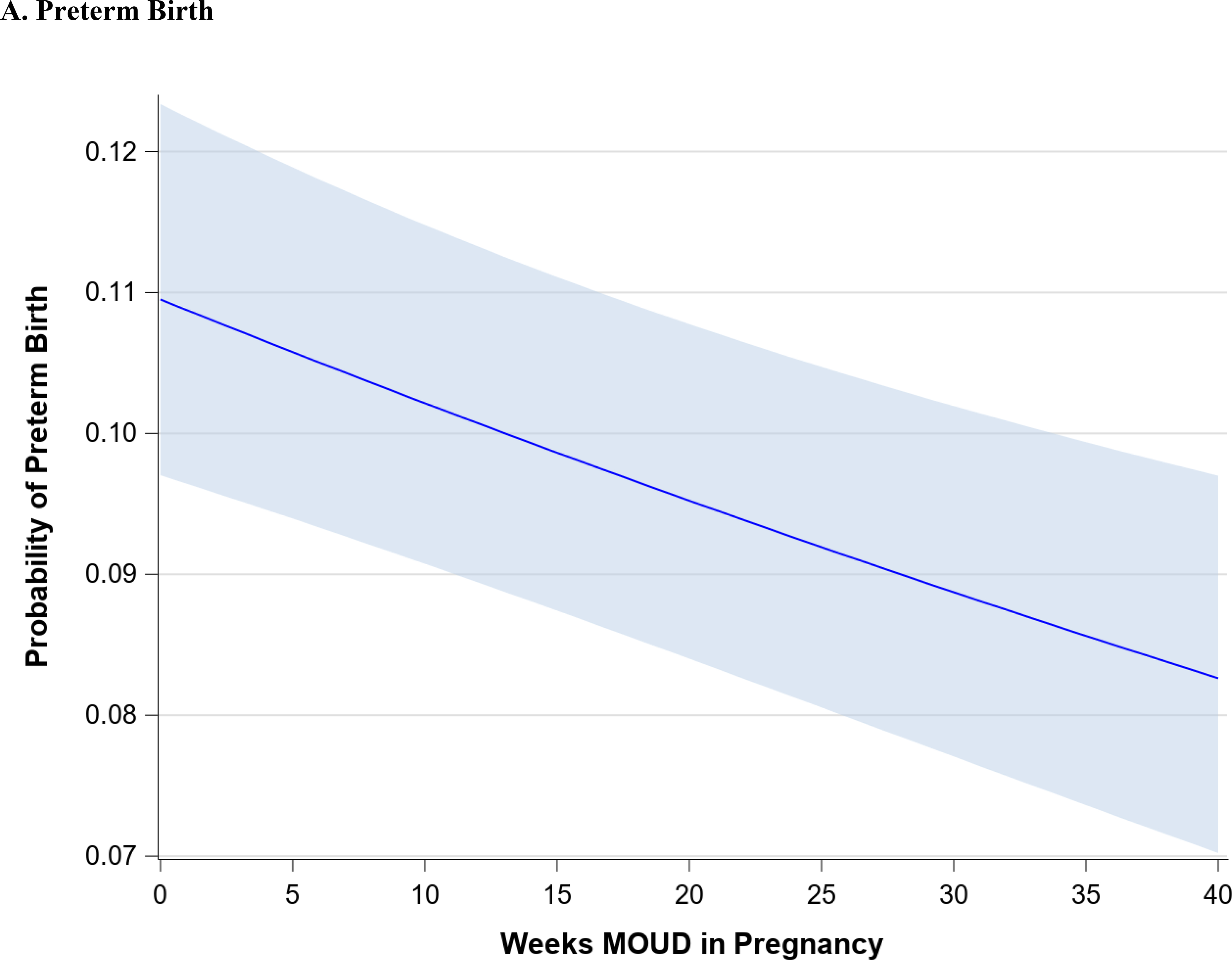
Among 13 320 pregnancies, 306 (2.3%) were complicated by an overdose, 1753 (13.2%) resulted in a preterm birth and 6787 (50.9%) continued MOUD postpartum. Among infants, 874 (7.6%) were low birth weight at term and 7706 (57.9%) were diagnosed with NAS. As the duration of MOUD use increased, we found a statistically significant decrease in the rate of overdose and preterm birth, a statistically significant increase in the rate of postpartum MOUD continuation and NAS and a decline in term low birth weight. Specifically, for each additional week of MOUD, the adjusted odds of overdose decreased by 2% [adjusted odds ratio (aOR) = 0.98; 95% confidence interval (CI) = 0.97, 0.99], preterm birth decreased by 1% (aOR = 0.99; 95% CI = 0.99, 1.00), postpartum MOUD continuation increased by 95% (aOR = 1.95; 95% CI = 1.87, 2.04) and NAS increased by 41% (aOR = 1.41; 95% CI = 1.35, 1.47). The odds of term low birth weight did not change (aOR = 1.00; 95% CI = 0.99, 1.00), although the rate declined with a longer duration of MOUD use during pregnancy.
Longer duration of medication for opioid use disorder use during pregnancy appears to be associated with improved maternal and perinatal outcomes.
检验妊娠期间阿片类药物使用障碍(MOUD)治疗持续时间对产妇、围产期和新生儿结局的影响。
基于索赔、就诊和药房数据的回顾性队列分析。
美国宾夕法尼亚州。
我们分析了 2009 年至 2017 年间,宾夕法尼亚州医疗补助计划中 10741 名年龄在 15-44 岁的阿片类药物使用障碍女性中的 13320 例妊娠,这些女性都接受了 MOUD 治疗。
我们在妊娠期间和产后 12 周内检测了五种结局:(1)过量用药,(2)产后 MOUD 持续使用,(3)早产(<37 周妊娠),(4)足月低体重(<2500 克,≥37 周)和(5)新生儿戒断综合征(NAS)。我们的主要暴露因素是妊娠期间任何 MOUD 治疗(包括美沙酮或丁丙诺啡)的持续时间(周数)。
在 13320 例妊娠中,306 例(2.3%)发生了用药过量,1753 例(13.2%)导致早产,6787 例(50.9%)产后继续 MOUD 治疗。在婴儿中,874 例(7.6%)足月出生体重低,7706 例(57.9%)诊断为 NAS。随着 MOUD 使用时间的增加,我们发现用药过量和早产的发生率呈统计学显著下降,产后 MOUD 持续使用和 NAS 的发生率呈统计学显著上升,足月低体重的发生率呈下降趋势。具体来说,MOUD 治疗每增加一周,用药过量的调整后比值比(aOR)下降 2%[调整后比值比(aOR)=0.98;95%置信区间(CI)=0.97,0.99],早产的调整后比值比下降 1%(aOR=0.99;95%CI=0.99,1.00),产后 MOUD 持续使用的调整后比值比增加 95%(aOR=1.95;95%CI=1.87,2.04),NAS 增加 41%(aOR=1.41;95%CI=1.35,1.47)。足月低体重的调整后比值比没有改变(aOR=1.00;95%CI=0.99,1.00),尽管随着 MOUD 治疗时间的延长,其发生率呈下降趋势。
妊娠期间阿片类药物使用障碍治疗时间延长似乎与改善产妇和围产期结局有关。