Dept. of Obstetrics, Gynecology & Reproductive Sciences, Yale School of Medicine, New Haven, CT, USA.
Section on Behavioral Endocrinology, National Institute of Mental Health, NIH, Bethesda, MD, USA.
Mol Psychiatry. 2021 Nov;26(11):6963-6974. doi: 10.1038/s41380-021-01144-8. Epub 2021 May 25.
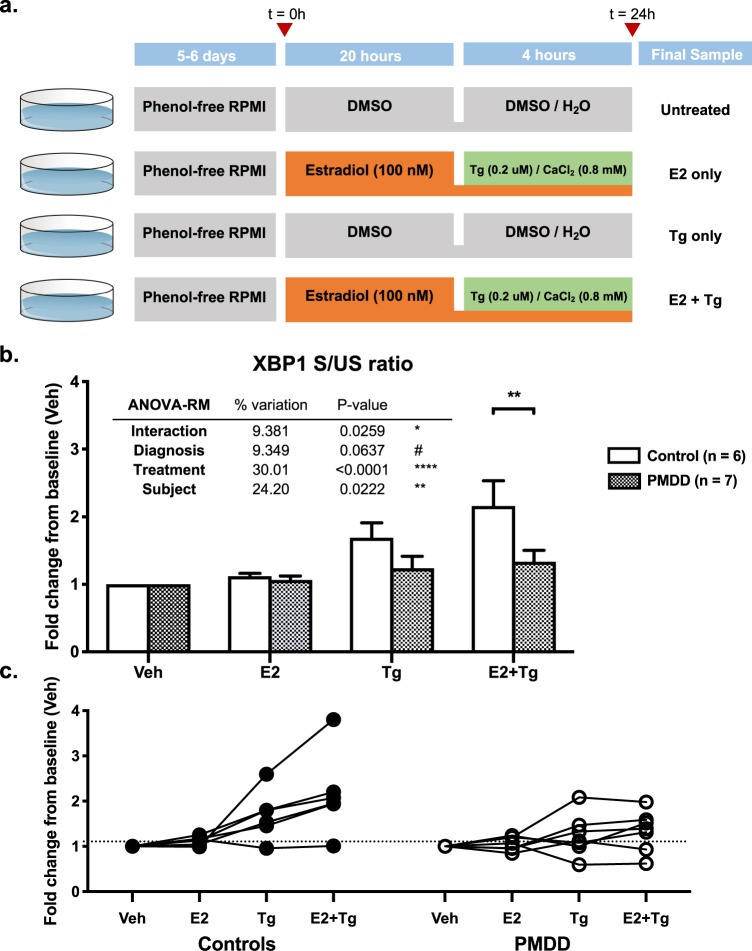
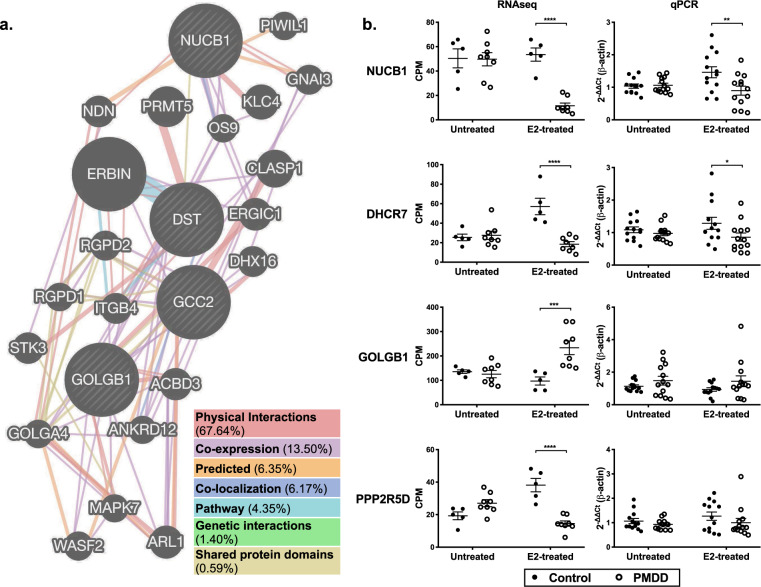
Premenstrual Dysphoric Disorder (PMDD) is characterized by debilitating mood symptoms in the luteal phase of the menstrual cycle. Prior studies of affected women have implicated a differential response to ovarian steroids. However, the molecular basis of these patients' differential response to hormone remains poorly understood. We performed transcriptomic analyses of lymphoblastoid cell lines (LCLs) derived from women with PMDD and asymptomatic controls cultured under untreated (steroid-free), estradiol-treated (E2), and progesterone-treated (P4) conditions. Weighted gene correlation network analysis (WGCNA) of transcriptomes identified four gene modules with significant diagnosis x hormone interactions, including one enriched for neuronal functions. Next, in a gene-level analysis comparing transcriptional response to hormone across diagnoses, a generalized linear model identified 1522 genes differentially responsive to E2 (E2-DRGs). Among the top 10 E2-DRGs was a physically interacting network (NUCB1, DST, GCC2, GOLGB1) involved in endoplasmic reticulum (ER)-Golgi function. qRT-PCR validation reproduced a diagnosis x E2 interaction (F(1,24)=7.01, p = 0.014) for NUCB1, a regulator of cellular Ca and ER stress. Finally, we used a thapsigargin (Tg) challenge assay to test whether E2 induces differences in Ca homeostasis and ER stress response in PMDD. PMDD LCLs had a 1.36-fold decrease in Tg-induced XBP1 splicing response compared to controls, and a 1.62-fold decreased response (p = 0.005), with a diagnosis x treatment interaction (F(3,33)=3.51, p = 0.026) in the E2-exposed condition. Altered hormone-dependent in cellular Ca dynamics and ER stress may contribute to the pathophysiology of PMDD.
经前期烦躁障碍 (PMDD) 的特征是在月经周期的黄体期出现使人虚弱的情绪症状。先前对受影响女性的研究表明,她们对卵巢类固醇的反应存在差异。然而,这些患者对激素的反应差异的分子基础仍知之甚少。我们对来自 PMDD 女性和无症状对照的淋巴母细胞系 (LCL) 进行了转录组分析,这些细胞在未经处理(无类固醇)、雌二醇处理 (E2) 和孕酮处理 (P4) 条件下培养。转录组的加权基因相关网络分析 (WGCNA) 鉴定了四个具有显著诊断与激素相互作用的基因模块,其中一个富含神经元功能。接下来,在比较跨诊断的激素转录反应的基因水平分析中,广义线性模型鉴定了 1522 个对 E2 有反应的基因 (E2-DRGs)。在 top10 E2-DRGs 中,有一个涉及内质网 (ER)-高尔基体功能的物理相互作用网络 (NUCB1、DST、GCC2、GOLGB1)。qRT-PCR 验证再现了 NUCB1 的诊断与 E2 相互作用 (F(1,24)=7.01, p=0.014),NUCB1 是细胞内 Ca 和 ER 应激的调节剂。最后,我们使用他普西他汀 (Tg) 挑战测定来测试 E2 是否在 PMDD 中诱导 Ca 动态平衡和 ER 应激反应的差异。与对照相比,PMDD LCL 在用 Tg 处理时 XBP1 剪接反应的诱导降低了 1.36 倍,反应降低了 1.62 倍(p=0.005),并且在 E2 暴露条件下存在诊断与处理的相互作用 (F(3,33)=3.51, p=0.026)。改变的激素依赖性细胞内 Ca 动力学和 ER 应激可能导致 PMDD 的病理生理学变化。