Liang Run-Bin, Zhao Yang, He Min-Ke, Wen Dong-Sheng, Bu Xiao-Yun, Huang Ye-Xing, Lai Zhi-Cheng, Xu Yu-Jie, Kan Anna, Wei Wei, Zhang Yao-Jun, Chen Min-Shan, Guo Rong-Ping, Li Qi-Jiong, Shi Ming
Department of Hepatobiliary Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
Front Oncol. 2021 May 12;11:619461. doi: 10.3389/fonc.2021.619461. eCollection 2021.
Our previous study showed that hepatic arterial infusion chemotherapy (HAIC) using oxaliplatin, fluorouracil, and leucovorin (FOLFOX) plus sorafenib provided a significant survival benefit over sorafenib for advanced hepatocellular carcinoma. However, it is unclear whether the survival benefit should be attributed to the synergism between HAIC and sorafenib or just HAIC alone. We aim to compare HAIC using FOLFOX plus sorafenib with HAIC alone in patients with advanced hepatocellular carcinoma.
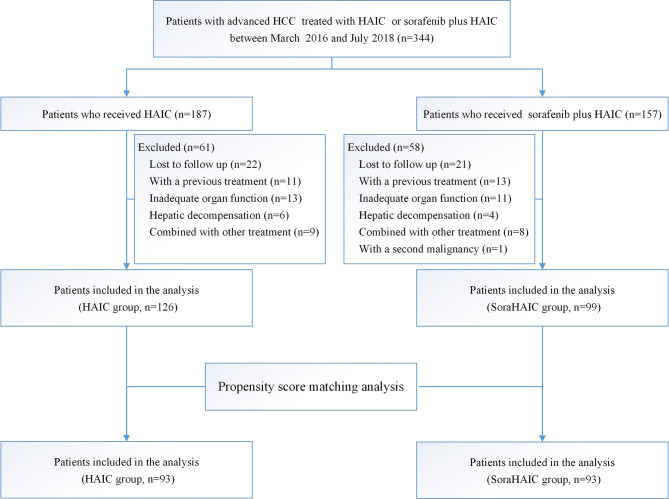
This was a retrospective study including 225 eligible patients treated with HAIC using FOLFOX (HAIC alone group, n=126, oxaliplatin 85 mg/m², leucovorin 400 mg/m², fluorouracil bolus 400 mg/m² and 2400 mg/m² for 46 hours, every 3 weeks) alone or HAIC plus sorafenib (soraHAIC group, n=99, sorafenib 400 mg twice daily). Survival curves were calculated by the Kaplan-Meier method, and propensity-score matching was used to reduce bias.
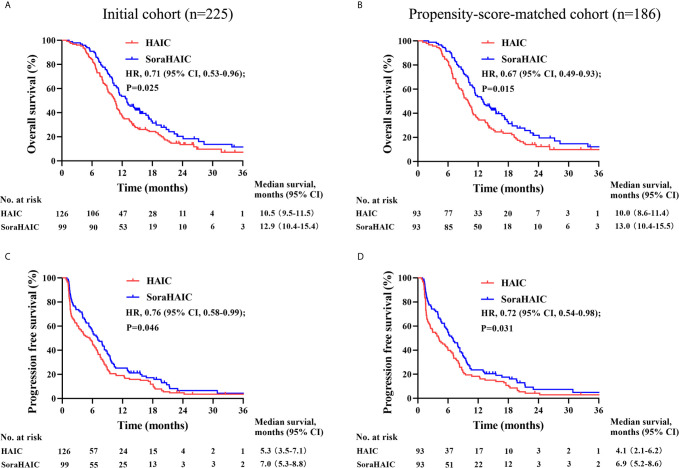
The soraHAIC group showed a longer overall survival (12.9 [95% CI, 10.4-15.4] vs. 10.5 [95% CI, 9.5-11.5] months, HR=0.71 [95% CI, 0.53-0.96]; =0.025), a better progression free survival (7.0 [95% CI, 5.3-8.8] vs. 5.3 [95% CI, 3.5-7.1] months, HR=0.76 [95% CI, 0.58-0.99]; =0.046), and a higher disease control rate (RECIST 1.1: 74.8% vs. 61.1%, =0.030) than the HAIC alone group. In multivariate analysis, soraHAIC was an independent favor factor for survival. In terms of the grade 3/4 adverse event, hand-foot skin reaction was more frequent in the soraHAIC group than the HAIC alone group. In the propensity-score matched cohorts (93 pairs), the overall survival, the progression free survival and disease control rates in the soraHAIC group were also better than those in the HAIC group (<0.05).
HAIC plus sorafenib may improve overall survival and progression free survival compared with HAIC alone as initial treatment for advanced hepatocellular carcinoma.
我们之前的研究表明,对于晚期肝细胞癌,使用奥沙利铂、氟尿嘧啶和亚叶酸钙(FOLFOX)的肝动脉灌注化疗(HAIC)联合索拉非尼比单独使用索拉非尼能带来显著的生存获益。然而,尚不清楚这种生存获益应归因于HAIC与索拉非尼之间的协同作用还是仅HAIC本身。我们旨在比较FOLFOX联合索拉非尼的HAIC与单独使用HAIC治疗晚期肝细胞癌患者的疗效。
这是一项回顾性研究,纳入了225例符合条件的患者,这些患者接受了单独使用FOLFOX的HAIC(单独HAIC组,n = 126,奥沙利铂85 mg/m²,亚叶酸钙400 mg/m²,氟尿嘧啶推注400 mg/m²并持续46小时输注2400 mg/m²,每3周一次)或HAIC联合索拉非尼(索拉非尼联合HAIC组,n = 99,索拉非尼400 mg,每日两次)治疗。通过Kaplan-Meier方法计算生存曲线,并使用倾向评分匹配来减少偏倚。
索拉非尼联合HAIC组的总生存期更长(12.9 [95% CI,10.4 - 15.4] 个月 vs. 10.5 [95% CI,9.5 - 11.5] 个月,HR = 0.71 [95% CI,0.53 - 0.96];P = 0.025),无进展生存期更好(7.0 [95% CI,5.3 - 8.8] 个月 vs. 5.3 [95% CI,3.5 - 7.1] 个月,HR = 0.76 [95% CI,0.58 - 0.99];P = 0.046),疾病控制率更高(根据RECIST 1.1标准:74.8% vs. 61.1%,P = 0.030),均优于单独HAIC组。在多因素分析中,索拉非尼联合HAIC是生存的独立有利因素。在3/4级不良事件方面,索拉非尼联合HAIC组的手足皮肤反应比单独HAIC组更常见。在倾向评分匹配队列(93对)中,索拉非尼联合HAIC组的总生存期、无进展生存期和疾病控制率也优于HAIC组(P < 0.05)。
作为晚期肝细胞癌的初始治疗,与单独使用HAIC相比,HAIC联合索拉非尼可能改善总生存期和无进展生存期。