Bjertnæs Lars J, Hindberg Kristian, Næsheim Torvind O, Suborov Evgeny V, Reierth Eirik, Kirov Mikhail Y, Lebedinskii Konstantin M, Tveita Torkjel
Anesthesia and Critical Care Research Group, University of Tromsø (UiT), The Arctic University of Norway, Tromsø, Norway.
K. G. Jebsen Thrombosis Research and Expertise Center, University of Tromsø (UiT), The Arctic University of Norway, Tromsø, Norway.
Front Med (Lausanne). 2021 May 13;8:641633. doi: 10.3389/fmed.2021.641633. eCollection 2021.
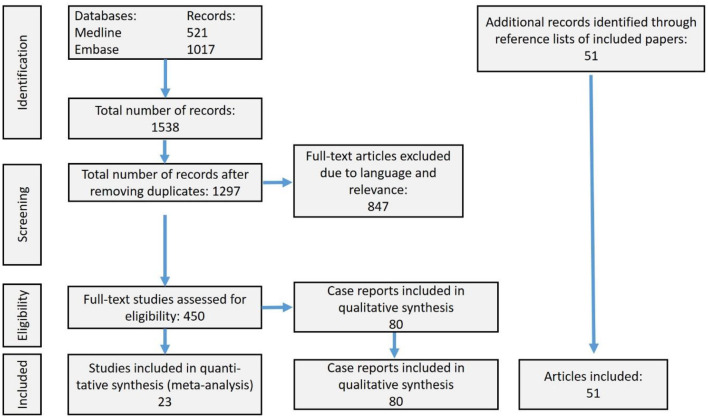
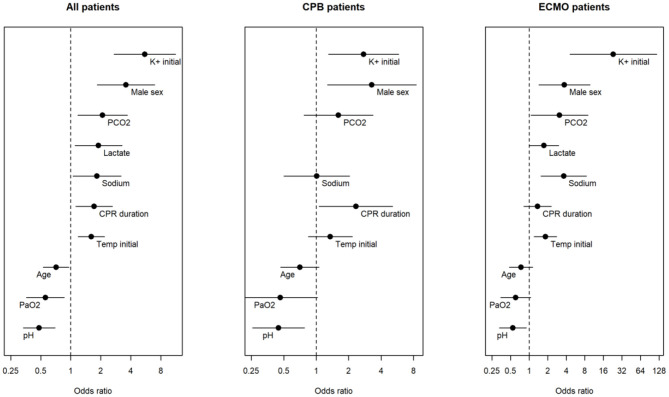
This systematic review and meta-analysis aims at comparing outcomes of rewarming after accidental hypothermic cardiac arrest (HCA) with cardiopulmonary bypass (CPB) or/and extracorporeal membrane oxygenation (ECMO). Literature searches were limited to references with an abstract in English, French or German. Additionally, we searched reference lists of included papers. Primary outcome was survival to hospital discharge. We assessed neurological outcome, differences in relative risks (RR) of surviving, as related to the applied rewarming technique, sex, asphyxia, and witnessed or unwitnessed HCA. We calculated hypothermia outcome prediction probability score after extracorporeal life support (HOPE) in patients in whom we found individual data. < 0.05 considered significant. Twenty-three case observation studies comprising 464 patients were included in a meta-analysis comparing outcomes of rewarming with CPB or/and ECMO. One-hundred-and-seventy-two patients (37%) survived to hospital discharge, 76 of 245 (31%) after CPB and 96 of 219 (44 %) after ECMO; 87 and 75%, respectively, had good neurological outcomes. Overall chance of surviving was 41% higher ( = 0.005) with ECMO as compared with CPB. A man and a woman had 46% ( = 0.043) and 31% ( = 0.115) higher chance, respectively, of surviving with ECMO as compared with CPB. Avalanche victims had the lowest chance of surviving, followed by drowning and people losing consciousness in cold environments. Assessed by logistic regression, asphyxia, unwitnessed HCA, male sex, high initial body temperature, low pH and high serum potassium (s-K) levels were associated with reduced chance of surviving. In patients displaying individual data, overall mean predictive surviving probability (HOPE score; = 134) was 33.9 ± 33.6% with no significant difference between ECMO and CPB-treated patients. We also surveyed 80 case reports with 96 victims of HCA, who underwent resuscitation with CPB or ECMO, without including them in the meta-analysis. The chance of surviving was significantly higher after rewarming with ECMO, as compared to CPB, and in patients with witnessed compared to unwitnessed HCA. Avalanche victims had the lowest probability of surviving. Male sex, high initial body temperature, low pH, and high s-K were factors associated with low surviving chances.
本系统评价和荟萃分析旨在比较意外低温心脏骤停(HCA)后采用体外循环(CPB)或/和体外膜肺氧合(ECMO)复温的效果。文献检索仅限于有英文、法文或德文摘要的参考文献。此外,我们还检索了纳入论文的参考文献列表。主要结局是存活至出院。我们评估了神经学结局、与应用的复温技术、性别、窒息以及目击或未目击的HCA相关的存活相对风险(RR)差异。我们计算了找到个体数据的患者体外生命支持后低温结局预测概率评分(HOPE)。<0.05被认为具有统计学意义。23项包含464例患者的病例观察研究纳入了一项比较CPB或/和ECMO复温效果的荟萃分析。172例患者(37%)存活至出院,CPB后245例中的76例(31%),ECMO后219例中的96例(44%);分别有87%和75%的患者神经学结局良好。与CPB相比,ECMO的总体存活机会高41%(P = 0.005)。与CPB相比,男性和女性接受ECMO复温后的存活机会分别高46%(P = 0.043)和31%(P = 0.115)。雪崩受害者的存活机会最低,其次是溺水者和在寒冷环境中失去意识的人。通过逻辑回归评估,窒息、未目击的HCA、男性、初始体温高、pH值低和血清钾(s-K)水平高与存活机会降低相关。在显示个体数据的患者中,总体平均预测存活概率(HOPE评分;P = 134)为33.9±33.6%,接受ECMO和CPB治疗的患者之间无显著差异。我们还调查了80篇病例报告,涉及96例接受CPB或ECMO复苏的HCA受害者,但未将其纳入荟萃分析。与CPB相比,ECMO复温后的存活机会显著更高,目击HCA的患者比未目击HCA的患者存活机会更高。雪崩受害者的存活概率最低。男性、初始体温高、pH值低和s-K高是与低存活机会相关的因素。