Genome Medical Sciences Project, National Center for Global Health and Medicine, Ichikawa 272-8516, Japan.
Department of Drug Development and Regulatory Science, Faculty of Pharmacy, Keio University, Tokyo 105-8512, Japan.
Int J Mol Sci. 2021 May 8;22(9):5000. doi: 10.3390/ijms22095000.
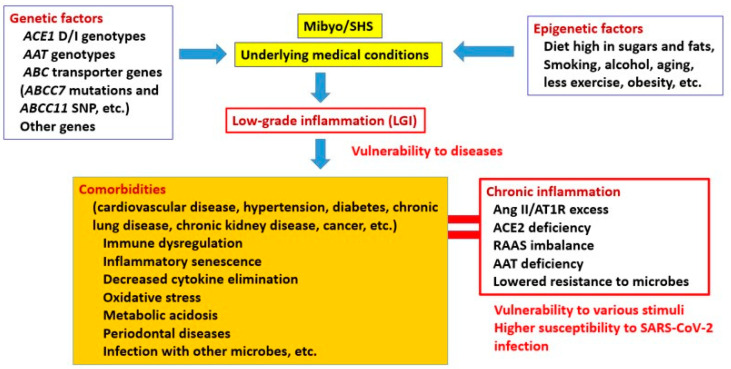
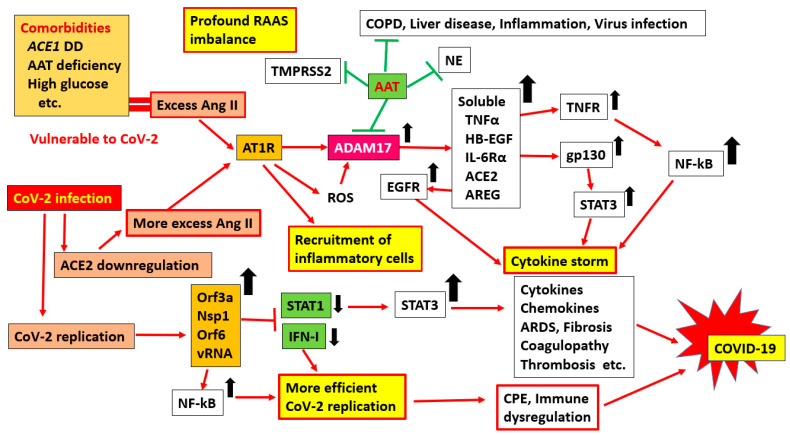
The elderly and patients with several comorbidities experience more severe cases of coronavirus disease 2019 (COVID-19) than healthy patients without underlying medical conditions. However, it is unclear why these people are prone to developing alveolar pneumonia, rapid exacerbations, and death. Therefore, we hypothesized that people with comorbidities may have a genetic predisposition that makes them more vulnerable to various factors; for example, they are likely to become more severely ill when infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). To test this hypothesis, we searched the literature extensively. Polymorphisms of genes, such as those that encode angiotensin-converting enzyme 1 (), have been associated with numerous comorbidities, such as cardiovascular disease, hypertension, diabetes, chronic kidney disease, and obesity, and there are potential mechanisms to explain these associations (e.g., DD-type carriers have greater ACE1 activity, and patients with a genetic alpha-1 anti-trypsin (AAT) deficiency lack control over inflammatory mediators). Since comorbidities are associated with chronic inflammation and are closely related to the renin-angiotensin-aldosterone system (RAAS), these individuals may already have a mild ACE1/ACE2 imbalance before viral infection, which increases their risk for developing severe cases of COVID-19. However, there is still much debate about the association between D/I polymorphism and comorbidities. The best explanation for this discrepancy could be that the D allele and DD subtypes are associated with comorbidities, but the DD genotype alone does not have an exceptionally large effect. This is also expected since the D/I polymorphism is only an intron marker. We also discuss how polymorphisms of and other genes are involved in comorbidities and the severity of SARS-CoV-2 infection. Presumably, a combination of multiple genes and non-genetic factors is involved in the establishment of comorbidities and aggravation of COVID-19.
老年人和患有多种合并症的患者比没有潜在医疗条件的健康患者经历更严重的 2019 年冠状病毒病(COVID-19)。然而,尚不清楚为什么这些人容易发生肺泡肺炎、快速恶化和死亡。因此,我们假设患有合并症的人可能具有遗传易感性,使他们更容易受到各种因素的影响;例如,当感染严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)时,他们更有可能病情加重。为了验证这一假设,我们广泛搜索了文献。编码血管紧张素转换酶 1()等基因的多态性与许多合并症有关,如心血管疾病、高血压、糖尿病、慢性肾脏病和肥胖症,并且有潜在的机制可以解释这些关联(例如,DD 型携带者的 ACE1 活性更高,而携带遗传型α-1 抗胰蛋白酶(AAT)缺乏症的患者缺乏对炎症介质的控制)。由于合并症与慢性炎症有关,并且与肾素-血管紧张素-醛固酮系统(RAAS)密切相关,因此这些个体在病毒感染前可能已经存在轻度 ACE1/ACE2 失衡,这增加了他们患严重 COVID-19 的风险。然而,关于 D/I 多态性与合并症之间的关联仍存在很多争议。造成这种差异的最佳解释可能是 D 等位基因和 DD 亚型与合并症有关,但 DD 基因型本身并没有特别大的影响。这也是意料之中的,因为 D/I 多态性只是一个内含子标记。我们还讨论了 和其他基因的多态性如何参与合并症和 SARS-CoV-2 感染的严重程度。据推测,多种基因和非遗传因素的组合参与了合并症的建立和 COVID-19 的恶化。