Oxford Uehiro Centre for Practical Ethics, Faculty of Philosophy, University of Oxford, Suite 8, Littlegate House, St Ebbes St, Oxford, OX1 1PT, UK.
Murdoch Children's Research Institute, Melbourne, Australia.
BMC Med Ethics. 2021 Jun 1;22(1):70. doi: 10.1186/s12910-021-00638-y.
ECMO is a particularly scarce resource during the COVID-19 pandemic. Its allocation involves ethical considerations that may be different to usual times. There is limited pre-pandemic literature on the ethical factors that ECMO physicians consider during ECMO allocation. During the pandemic, there has been relatively little professional guidance specifically relating to ethics and ECMO allocation; although there has been active ethical debate about allocation of other critical care resources. We report the results of a small international exploratory survey of ECMO clinicians' views on different patient factors in ECMO decision-making prior to and during the COVID-19 pandemic. We then outline current ethical decision procedures and recommendations for rationing life-sustaining treatment during the COVID-19 pandemic, and examine the extent to which current guidelines for ECMO allocation (and reported practice) adhere to these ethical guidelines and recommendations.
An online survey was performed with responses recorded between mid May and mid August 2020. Participants (n = 48) were sourced from the ECMOCard study group-an international group of experts (n = 120) taking part in a prospective international study of ECMO and intensive care for patients during the COVID-19 pandemic. The survey compared the extent to which certain ethical factors involved in ECMO resource allocation were considered prior to and during the pandemic.
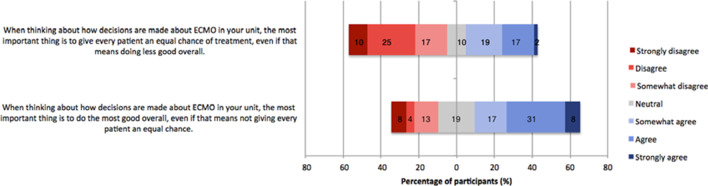
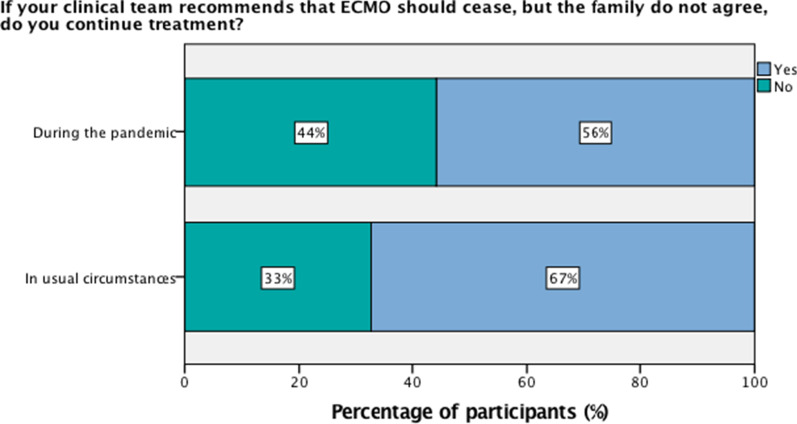
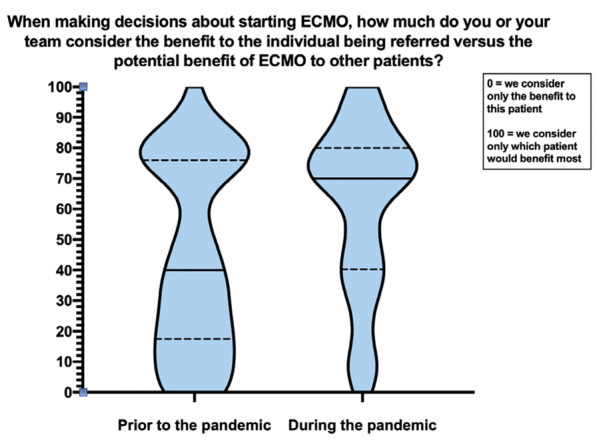
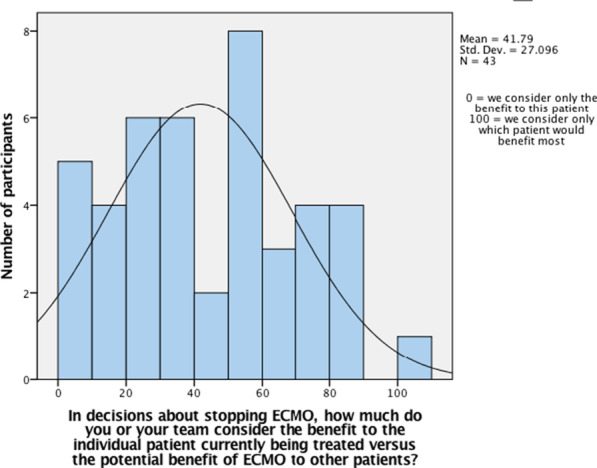
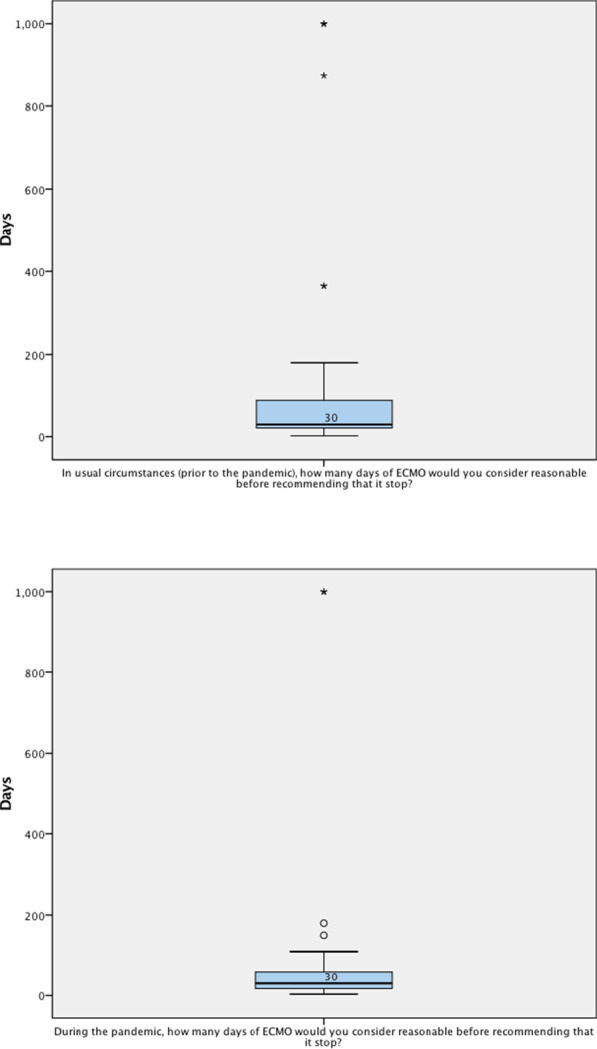
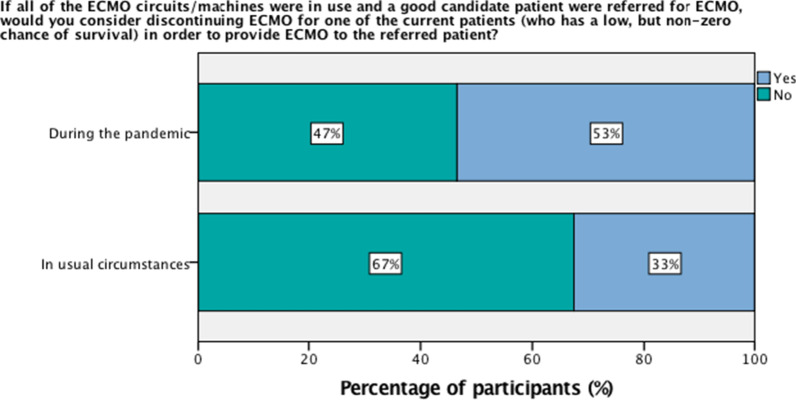
When initiating ECMO during the pandemic, compared to usual times, participants reported giving more ethical weight to the benefit of ECMO to other patients not yet admitted as opposed to those already receiving ECMO, (p < 0.001). If a full unit were referred a good candidate for ECMO, participants were more likely during the pandemic to consider discontinuing ECMO from a current patient with low chance of survival (53% during pandemic vs. 33% prior p = 0.002). If the clinical team recommends that ECMO should cease, but family do not agree, the majority of participants indicated that they would continue treatment, both in usual circumstances (67%) and during the pandemic (56%).
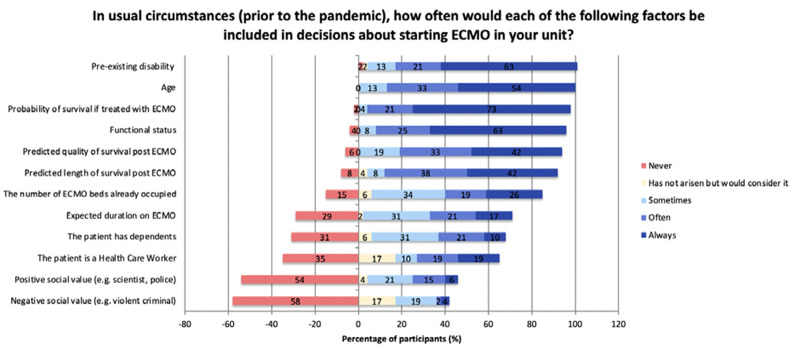
We found differences during the COVID-19 pandemic in prioritisation of several ethical factors in the context of ECMO allocation. The ethical principles prioritised by survey participants were largely consistent with ECMO allocation guidelines, current ethical decision procedures and recommendations for allocation of life-sustaining treatment during the COVID-19 pandemic.
在 COVID-19 大流行期间,ECMO 是一种特别稀缺的资源。其分配涉及到可能与往常不同的伦理考虑。在大流行之前,关于 ECMO 医生在 ECMO 分配过程中考虑的伦理因素的文献有限。在大流行期间,虽然关于其他关键医疗资源分配的伦理辩论非常活跃,但几乎没有专门针对伦理和 ECMO 分配的专业指导。我们报告了一项针对 ECMO 临床医生在 COVID-19 大流行之前和期间对 ECMO 决策中不同患者因素的看法的小型国际探索性调查的结果。然后,我们概述了 COVID-19 大流行期间维持生命治疗的定量配给的当前伦理决策程序和建议,并研究了当前 ECMO 分配指南(和报告的实践)在多大程度上遵守这些伦理指南和建议。
2020 年 5 月中旬至 8 月中旬期间进行了在线调查,并记录了参与者的回复。参与者(n=48)来自 ECMOCard 研究小组-一个由参与 COVID-19 大流行期间 ECMO 和重症监护患者的前瞻性国际研究的专家(n=120)组成的国际专家组。该调查比较了在大流行期间和往常时期,在 ECMO 资源分配中涉及的某些伦理因素的考虑程度。
在大流行期间启动 ECMO 时,与往常时期相比,参与者报告说,与已经接受 ECMO 的患者相比,更重视 ECMO 对尚未入院的其他患者的益处(p<0.001)。如果一个完整的单位被推荐为 ECMO 的好候选人,那么在大流行期间,参与者更有可能考虑停止当前生存机会低的患者的 ECMO(53%在大流行期间,而 33%在大流行前,p=0.002)。如果临床团队建议停止 ECMO,但家属不同意,大多数参与者表示,他们将继续治疗,无论是在常规情况下(67%)还是在大流行期间(56%)。
我们发现,在 COVID-19 大流行期间,在 ECMO 分配背景下,对几个伦理因素的优先级排序存在差异。调查参与者优先考虑的伦理原则在很大程度上与 ECMO 分配指南、当前的伦理决策程序以及 COVID-19 大流行期间维持生命治疗的分配建议一致。