Rabie Ahmed A, Elhazmi Alyaa, Azzam Mohamed H, Abdelbary Akram, Labib Ahmed, Combes Alain, Zakhary Bishoy, MacLaren Graeme, Barbaro Ryan P, Peek Giles J, Antonini Marta Velia, Shekar Kiran, Al-Fares Abdulrahman, Oza Pranay, Mehta Yatin, Alfoudri Huda, Ramanathan Kollengode, Ogino Mark, Raman Lakshmi, Paden Matthew, Brodie Daniel, Bartlett Robert
Critical Care Department-ECMO care Unit (ECU), Riyadh Region Cluster1, King Saud Medical City, Riyadh, Saudi Arabia.
Internal Medicine Department, King Faisal University, Riyadh, Saudi Arabia.
Ann Intensive Care. 2023 May 2;13(1):36. doi: 10.1186/s13613-023-01126-9.
The high-quality evidence on managing COVID-19 patients requiring extracorporeal membrane oxygenation (ECMO) support is insufficient. Furthermore, there is little consensus on allocating ECMO resources when scarce. The paucity of evidence and the need for guidance on controversial topics required an international expert consensus statement to understand the role of ECMO in COVID-19 better. Twenty-two international ECMO experts worldwide work together to interpret the most recent findings of the evolving published research, statement formulation, and voting to achieve consensus.
To guide the next generation of ECMO practitioners during future pandemics on tackling controversial topics pertaining to using ECMO for patients with COVID-19-related severe ARDS.
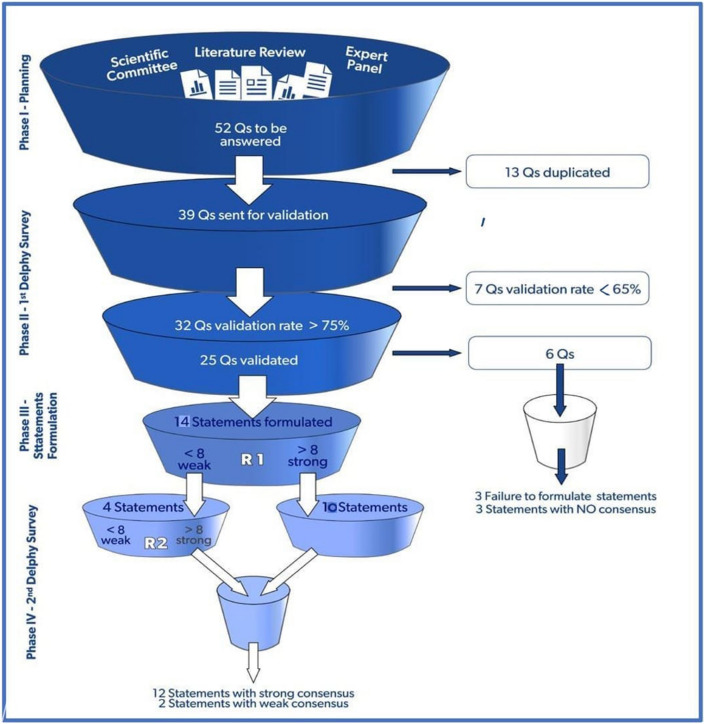
The scientific committee was assembled of five chairpersons with more than 5 years of ECMO experience and a critical care background. Their roles were modifying and restructuring the panel's questions and, assisting with statement formulation in addition to expert composition and literature review. Experts are identified based on their clinical experience with ECMO (minimum of 5 years) and previous academic activity on a global scale, with a focus on diversity in gender, geography, area of expertise, and level of seniority. We used the modified Delphi technique rounds and the nominal group technique (NGT) through three face-to-face meetings and the voting on the statement was conducted anonymously. The entire process was planned to be carried out in five phases: identifying the gap of knowledge, validation, statement formulation, voting, and drafting, respectively.
In phase I, the scientific committee obtained 52 questions on controversial topics in ECMO for COVID-19, further reviewed for duplication and redundancy in phase II, resulting in nine domains with 32 questions with a validation rate exceeding 75% (Fig. 1). In phase III, 25 questions were used to formulate 14 statements, and six questions achieved no consensus on the statements. In phase IV, two voting rounds resulted in 14 statements that reached a consensus are included in four domains which are: patient selection, ECMO clinical management, operational and logistics management, and ethics.
Three years after the onset of COVID-19, our understanding of the role of ECMO has evolved. However, it is incomplete. Tota14 statements achieved consensus; included in four domains discussing patient selection, clinical ECMO management, operational and logistic ECMO management and ethics to guide next-generation ECMO providers during future pandemic situations.
关于管理需要体外膜肺氧合(ECMO)支持的新冠肺炎患者的高质量证据不足。此外,在资源稀缺时如何分配ECMO资源也几乎没有共识。证据的匮乏以及对有争议话题指导的需求,需要一份国际专家共识声明,以更好地理解ECMO在新冠肺炎中的作用。全球22位国际ECMO专家共同努力,解读不断发展的已发表研究的最新发现,制定声明并进行投票以达成共识。
指导下一代ECMO从业者在未来大流行期间应对与使用ECMO治疗新冠肺炎相关严重急性呼吸窘迫综合征(ARDS)患者有关的争议性话题。
科学委员会由五位具有超过5年ECMO经验和重症监护背景的主席组成。他们的职责是修改和重组小组的问题,并协助制定声明,此外还负责专家组成和文献综述。专家是根据他们在ECMO方面的临床经验(至少5年)以及之前在全球范围内的学术活动来确定的,重点关注性别、地域、专业领域和资历水平的多样性。我们通过三次面对面会议使用了改良德尔菲技术轮次和名义小组技术(NGT),并对声明进行匿名投票。整个过程计划分五个阶段进行:分别是确定知识差距、验证、声明制定、投票和起草。
在第一阶段,科学委员会获得了52个关于新冠肺炎ECMO争议性话题的问题,在第二阶段进一步审查重复和冗余问题,结果形成了9个领域的32个问题,验证率超过75%(图1)。在第三阶段,25个问题被用于制定14条声明,有6个问题在声明上未达成共识。在第四阶段,两轮投票产生了14条达成共识的声明,涵盖四个领域,即:患者选择、ECMO临床管理、运营和后勤管理以及伦理。
新冠肺炎疫情爆发三年后,我们对ECMO作用的理解有所发展。然而,并不完整。共有14条声明达成共识;涵盖四个领域,讨论患者选择、ECMO临床管理、ECMO运营和后勤管理以及伦理,以指导下一代ECMO提供者应对未来大流行情况。