Department of Epidemiology, University of Florida College of Public Health and Health Professions, Gainesville, Florida.
University of Florida Health Cancer Center, Gainesville, Florida.
Cancer Epidemiol Biomarkers Prev. 2021 Aug;30(8):1582-1590. doi: 10.1158/1055-9965.EPI-21-0152. Epub 2021 Jun 2.
Previous reports suggested risk of death and breast cancer varied by comorbidity and age in older women undergoing mammography. However, impacts of functional limitations remain unclear.
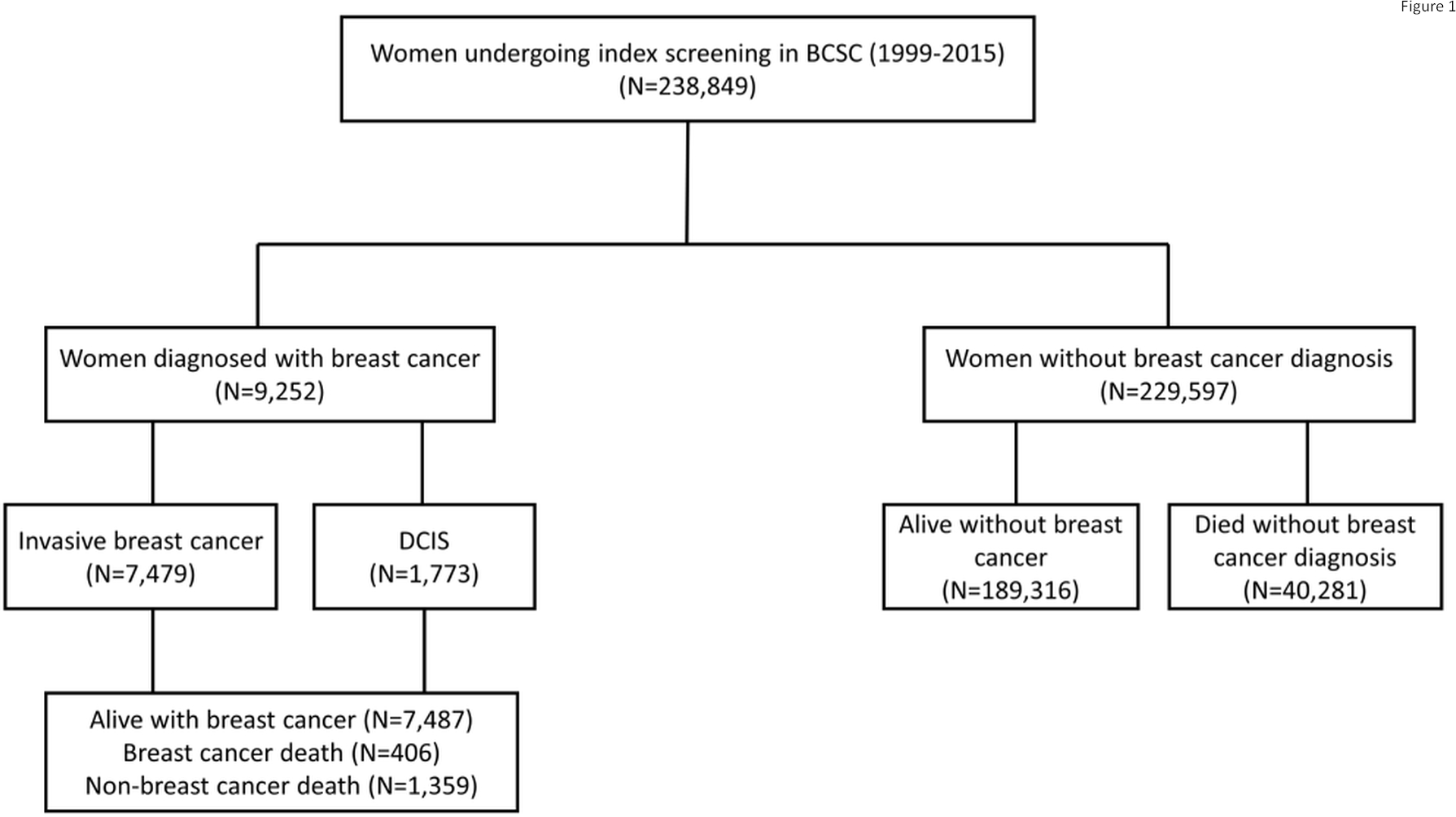
We used data from 238,849 women in the Breast Cancer Surveillance Consortium-Medicare linked database (1999-2015) who had screening mammogram at ages 66-94 years. We estimated risk of breast cancer, breast cancer death, and non-breast cancer death by function-related indicator (FRI) which incorporated 16 claims-based items and was categorized as an ordinal variable (0, 1, and 2+). Fine and Gray proportional sub-distribution hazards models were applied with breast cancer and death treated as competing events. Risk estimates by FRI scores were adjusted by age and NCI comorbidity index separately and stratified by these factors.
Overall, 9,252 women were diagnosed with breast cancer, 406 died of breast cancer, and 41,640 died from non-breast cancer causes. The 10-year age-adjusted invasive breast cancer risk slightly decreased with FRI score [FRI = 0: 4.0%, 95% confidence interval (CI) = 3.8-4.1; FRI = 1: 3.9%, 95% CI = 3.7-4.2; FRI ≥ 2: 3.5%, 95% CI = 3.1-3.9). Risk of non-breast cancer death increased with FRI score (FRI = 0: 18.8%, 95% CI = 18.5-19.1; FRI = 1: 24.4%, 95% CI = 23.9-25.0; FRI ≥ 2: 39.8%, 95% CI = 38.8-40.9]. Risk of breast cancer death was low with minimal differences across FRI scores. NCI comorbidity index-adjusted models and stratified analyses yielded similar patterns.
Risk of non-breast cancer death substantially increases with FRI score, whereas risk of breast cancer death is low regardless of functional status.
Older women with functional limitations should be informed that they may not benefit from screening mammography.
先前的报告表明,在接受乳房 X 光检查的老年女性中,合并症和年龄会影响死亡率和乳腺癌风险。然而,功能障碍的影响仍不清楚。
我们使用了来自乳腺癌监测联合会-医疗保险关联数据库(1999-2015 年)的 238849 名年龄在 66-94 岁之间接受筛查性乳房 X 光检查的女性的数据。我们通过包含 16 项基于索赔的项目的功能相关指标(FRI)来估计乳腺癌、乳腺癌死亡和非乳腺癌死亡的风险,FRI 被归类为有序变量(0、1 和 2+)。采用 Fine 和 Gray 比例亚分布风险模型,将乳腺癌和死亡视为竞争事件。通过 FRI 评分调整的风险估计值分别按年龄和 NCI 合并症指数进行调整,并按这些因素进行分层。
总体而言,9252 名女性被诊断患有乳腺癌,406 名女性死于乳腺癌,41640 名女性死于非乳腺癌原因。经过年龄调整后,10 年的侵袭性乳腺癌风险随着 FRI 评分的降低而略有下降[FRI = 0:4.0%,95%置信区间(CI)= 3.8-4.1;FRI = 1:3.9%,95%CI = 3.7-4.2;FRI≥2:3.5%,95%CI = 3.1-3.9]。非乳腺癌死亡风险随着 FRI 评分的增加而增加(FRI = 0:18.8%,95%CI = 18.5-19.1;FRI = 1:24.4%,95%CI = 23.9-25.0;FRI≥2:39.8%,95%CI = 38.8-40.9]。乳腺癌死亡风险较低,FRI 评分差异极小。NCI 合并症指数调整模型和分层分析得出了相似的结果。
非乳腺癌死亡风险随着 FRI 评分的增加而显著增加,而无论功能状态如何,乳腺癌死亡风险都很低。
功能受限的老年女性应被告知,她们可能不会从乳房 X 光筛查中受益。