Department of Orthopaedic Surgery, Nagoya University Graduate School of Medicine, 65 Tsurumai-cho, Showa-ku, Nagoya, Aichi, 466-8550, Japan.
Department of Orthopaedic Surgery, Chubu Rosai Hospital, 1-10-6, Komei-cho, Minami-ku, Nagoya, Aichi, 455-8530, Japan.
Sci Rep. 2021 Jun 2;11(1):11630. doi: 10.1038/s41598-021-91225-z.
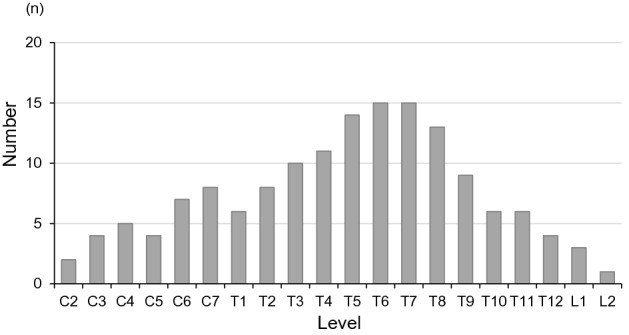
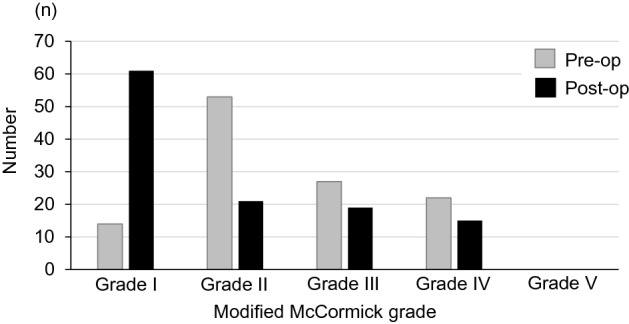
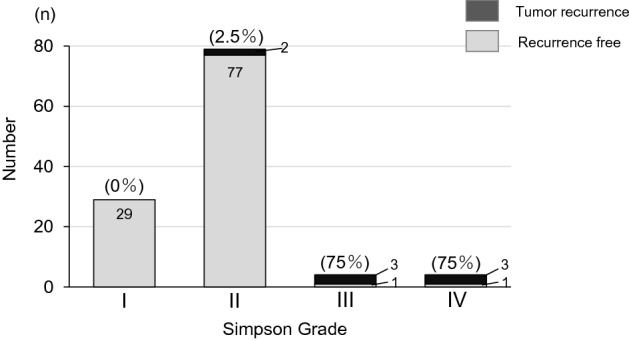
Meningiomas are benign tumors that are treated surgically. Local recurrence is likely if the dura is preserved, and en bloc tumor and dura resection (Simpson grade I) is recommended. In some cases the dura is cauterized and preserved after tumor resection (Simpson grade II). The purpose of this study was performed to analyze clinical features and prognostic factors associated with spinal meningioma, and to identify the most effective surgical treatment. The subjects were 116 patients (22 males, 94 females) with spinal meningioma who underwent surgery at seven NSG centers between 1998 and 2018. Clinical data were collected from the NSG database. Pre- and postoperative neurological status was defined using the modified McCormick scale. The patients had a mean age of 61.2 ± 14.8 years (range 19-91 years) and mean symptom duration of 11.3 ± 14.7 months (range 1-93 months). Complete resection was achieved in 108 cases (94%), including 29 Simpson grade I and 79 Simpson grade II resections. The mean follow-up period was 84.8 ± 52.7 months. At the last follow-up, neurological function had improved in 73 patients (63%), was stable in 34 (29%), and had worsened in 9 (8%). Eight patients had recurrence, and recurrence rates did not differ significantly between Simpson grades I and II in initial surgery. Kaplan-Meier analysis of recurrence-free survival showed that Simpson grade III or IV, male, and dural tail sign were significant factors associated with recurrence (P < 0.05). In conclusion, Simpson I resection is anatomically favorable for spinal meningiomas. Younger male patients with a dural tail and a high-grade tumor require close follow-up. The tumor location and feasibility of surgery can affect the surgical morbidity in Simpson I or II resection. All patients should be carefully monitored for long-term outcomes, and we recommend lifelong surveillance after surgery.
脑膜瘤是良性肿瘤,通常采用手术治疗。如果保留硬脑膜,肿瘤可能会局部复发,因此建议整块切除肿瘤和硬脑膜(Simpson 分级 I)。在某些情况下,肿瘤切除后硬脑膜会被烧灼并保留(Simpson 分级 II)。本研究旨在分析与脊髓脑膜瘤相关的临床特征和预后因素,并确定最有效的手术治疗方法。研究对象为 1998 年至 2018 年间在 7 个 NSG 中心接受手术治疗的 116 例(22 例男性,94 例女性)脊髓脑膜瘤患者。临床资料来自 NSG 数据库。术前和术后神经状态采用改良 McCormick 量表进行定义。患者平均年龄为 61.2±14.8 岁(19-91 岁),平均症状持续时间为 11.3±14.7 个月(1-93 个月)。108 例(94%)患者达到完全切除,其中 29 例为 Simpson 分级 I,79 例为 Simpson 分级 II。平均随访时间为 84.8±52.7 个月。末次随访时,73 例(63%)患者神经功能改善,34 例(29%)患者稳定,9 例(8%)患者恶化。8 例患者复发,初次手术中 Simpson 分级 I 和 II 之间的复发率无显著差异。无复发生存率的 Kaplan-Meier 分析显示,Simpson 分级 III 或 IV、男性和硬脑膜尾征是与复发相关的显著因素(P<0.05)。综上所述,Simpson I 级切除对脊髓脑膜瘤解剖有利。年轻的男性患者伴有硬脑膜尾和高级别肿瘤需要密切随访。肿瘤位置和手术可行性会影响 Simpson I 级或 II 级切除的手术发病率。所有患者都应密切监测长期结果,我们建议术后终身随访。