Austrian Institute for Health Technology Assessment (AIHTA), Vienna, Austria.
Austrian Institute for Health Technology Assessment (AIHTA), Vienna, Austria.
ESMO Open. 2021 Jun;6(3):100166. doi: 10.1016/j.esmoop.2021.100166. Epub 2021 Jun 1.
The magnitude of clinical benefit of solid cancer drugs can be standardly assessed via the Magnitude of Clinical Benefit Scale (MCBS) developed by the European Society for Medical Oncology (ESMO). We applied two ESMO-MCBS versions to the last 12 years of European cancer drug approval and compared two predefined marketing authorisation timeframes to identify potential score changes over time.
Originator solid cancer drugs and indication extensions that were approved between 1 January 2009 and 31 October 2020 by the European Medicines Agency (EMA) were included in our analyses. To evaluate the clinical benefit of these cancer indications, the original ESMO-MCBS (v 1.1) and a locally adapted ESMO-MCBS version were applied to the study sample. Thus, two ESMO-MCBS versions were compared, and an additional analysis was conducted to identify potential score differences between two approval timeframes 2009-2014 versus 2015-2020.
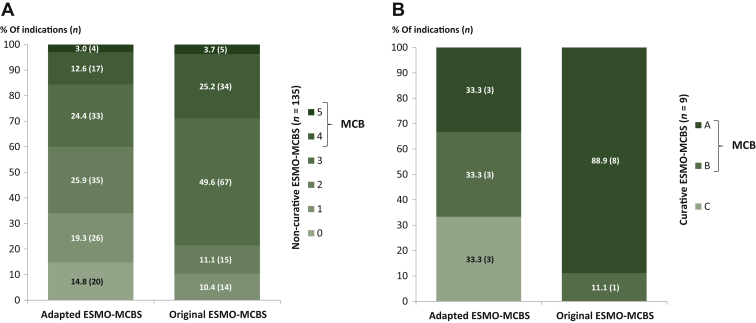
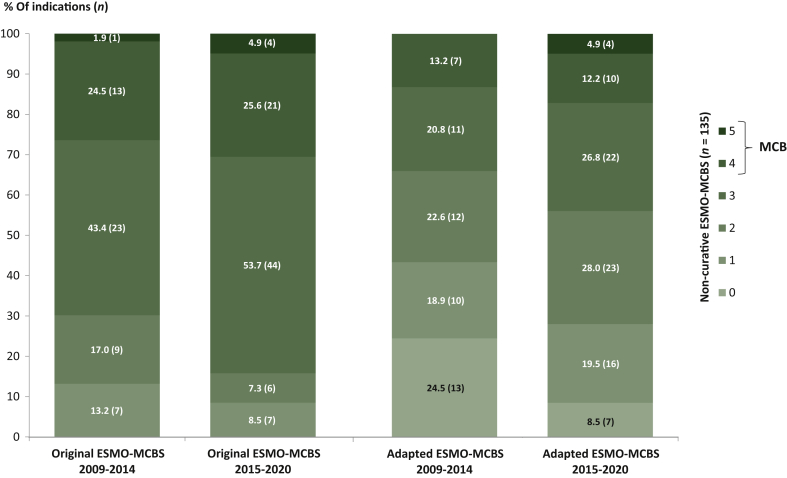
A total of 144 cancer indications intended as curative (n = 9) or non-curative (n = 135) treatment options were eligible for an ESMO-MCBS assessment. Solely a minority of the assessed cancer indications met the meaningful clinical benefit (MCB) criteria independent of the applied version of the scale and treatment intention (original: n = 48/144, 33.3% versus adapted: n = 27/144, 18.8%). Comparing the two EMA approval timeframes, a growing number of approved cancer indications could be observed: 2009-2014: n = 9/year versus 2015-2020: n = 14/year. In addition, almost no difference in the proportion of cancer indications that have met the MCB criteria was detectable when comparing the predefined authorisation timeframes (MCB increase original: +4.1% and adapted: +3.9%).
Applying both versions of the ESMO-MCBS can help to identify potentially beneficial cancer indications, but also those with rather uncertain or low clinical benefit and thus, support the fair allocation of limited health care resources.
欧洲肿瘤内科学会(ESMO)开发的临床获益量表(MCBS)可用于标准评估实体瘤药物的临床获益程度。我们将两种 ESMO-MCBS 版本应用于过去 12 年的欧洲癌症药物审批,并比较了两个预先设定的营销授权时间框架,以确定随着时间的推移潜在的评分变化。
纳入了 2009 年 1 月 1 日至 2020 年 10 月 31 日期间,由欧洲药品管理局(EMA)批准的原创实体瘤药物和适应症扩展的研究样本。为了评估这些癌症适应证的临床获益,我们将原始 ESMO-MCBS(版本 1.1)和本地改编的 ESMO-MCBS 版本应用于研究样本。因此,我们比较了两种 ESMO-MCBS 版本,并进行了额外的分析,以确定两个批准时间框架(2009-2014 年与 2015-2020 年)之间潜在的评分差异。
共有 144 种用于治疗(n=9)或非治疗(n=135)的癌症适应证符合 ESMO-MCBS 评估标准。仅少数评估的癌症适应证符合有意义的临床获益(MCB)标准,而与应用的量表版本和治疗意图无关(原始:n=48/144,33.3%与改编:n=27/144,18.8%)。比较两个 EMA 批准时间框架,可观察到批准的癌症适应证数量不断增加:2009-2014 年:n=9/年与 2015-2020 年:n=14/年。此外,当比较预先设定的授权时间框架时,几乎没有检测到符合 MCB 标准的癌症适应证比例有差异(原始:+4.1%和改编:+3.9%)。
应用 ESMO-MCBS 的两个版本可以帮助识别潜在有益的癌症适应证,也可以识别那些临床获益程度不确定或较低的癌症适应证,从而支持公平分配有限的医疗保健资源。