Department of Nephrology, Vall d'Hebron University Hospital, Vall d'Hebron Institute of Research, Vall d'Hebron Barcelona Hospital Campus, Red de Investigación Renal (REDINREN), Barcelona, Spain.
Department of Internal Medicine, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Clin J Am Soc Nephrol. 2021 Jul;16(7):1061-1072. doi: 10.2215/CJN.18961220. Epub 2021 Jun 4.
There is concern about potential deleterious effects of angiotensin-converting enzyme inhibitors (ACEis) and angiotensin II receptor blockers (ARBs) in patients with coronavirus disease 2019 (COVID-19). Patients with kidney failure, who often use ACEis/ARBs, are at higher risk of more severe COVID-19. However, there are no data available on the association of ACEi/ARB use with COVID-19 severity in this population.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: From the European Renal Association COVID-19 database (ERACODA), we retrieved data on kidney transplant recipients and patients on dialysis who were affected by COVID-19, between February 1 and October 1, 2020, and had information on 28-day mortality. We used Cox proportional-hazards regression to calculate hazard ratios for the association between ACEi/ARB use and 28-day mortality risk. Additionally, we studied the association of discontinuation of these agents with 28-day mortality.
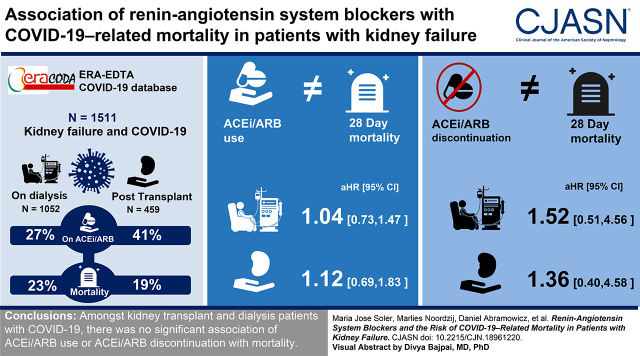
We evaluated 1511 patients: 459 kidney transplant recipients and 1052 patients on dialysis. At diagnosis of COVID-19, 189 (41%) of the transplant recipients and 288 (27%) of the patients on dialysis were on ACEis/ARBs. A total of 88 (19%) transplant recipients and 244 (23%) patients on dialysis died within 28 days of initial presentation. In both groups of patients, there was no association between ACEi/ARB use and 28-day mortality in both crude and adjusted models (in transplant recipients, adjusted hazard ratio, 1.12; 95% confidence interval [95% CI], 0.69 to 1.83; in patients on dialysis, adjusted hazard ratio, 1.04; 95% CI, 0.73 to 1.47). Among transplant recipients, ACEi/ARB discontinuation was associated with a higher mortality risk after adjustment for demographics and comorbidities, but the association was no longer statistically significant after adjustment for severity of COVID-19 (adjusted hazard ratio, 1.36; 95% CI, 0.40 to 4.58). Among patients on dialysis, ACEi/ARB discontinuation was not associated with mortality in any model. We obtained similar results across subgroups when ACEis and ARBs were studied separately, and when other outcomes for severity of COVID-19 were studied, , hospital admission, admission to the intensive care unit, or need for ventilator support.
Among kidney transplant recipients and patients on dialysis with COVID-19, there was no significant association of ACEi/ARB use or discontinuation with mortality.
人们担心血管紧张素转换酶抑制剂(ACEi)和血管紧张素 II 受体阻滞剂(ARB)在 2019 年冠状病毒病(COVID-19)患者中可能产生有害影响。经常使用 ACEi/ARB 的肾衰竭患者患 COVID-19 的风险更高,病情也更严重。然而,目前尚无关于该人群中 ACEi/ARB 使用与 COVID-19 严重程度之间关联的相关数据。
设计、设置、参与者和测量方法:我们从欧洲肾脏协会 COVID-19 数据库(ERACODA)中检索了 2020 年 2 月 1 日至 10 月 1 日期间患有 COVID-19 的肾移植受者和透析患者的数据,并记录了 28 天死亡率。我们使用 Cox 比例风险回归计算 ACEi/ARB 使用与 28 天死亡率风险之间的关联的风险比。此外,我们还研究了这些药物的停药与 28 天死亡率之间的关系。
我们评估了 1511 名患者:459 名肾移植受者和 1052 名透析患者。在 COVID-19 诊断时,459 名肾移植受者中有 189 名(41%)和 1052 名透析患者中有 288 名(27%)正在使用 ACEi/ARB。在初次就诊后的 28 天内,共有 88 名(19%)肾移植受者和 244 名(23%)透析患者死亡。在两组患者中,在未调整和调整后的模型中,ACEi/ARB 的使用均与 28 天死亡率无关(在肾移植受者中,调整后的危险比为 1.12;95%置信区间[95%CI]为 0.69 至 1.83;在透析患者中,调整后的危险比为 1.04;95%CI 为 0.73 至 1.47)。在肾移植受者中,ACEi/ARB 停药与调整人口统计学和合并症后的死亡率风险较高相关,但在调整 COVID-19 严重程度后,该关联不再具有统计学意义(调整后的危险比为 1.36;95%CI 为 0.40 至 4.58)。在透析患者中,在任何模型中,ACEi/ARB 停药均与死亡率无关。当分别研究 ACEi 和 ARB 以及研究 COVID-19 严重程度的其他结局(住院、入住重症监护病房或需要呼吸机支持)时,我们在亚组中得到了类似的结果。
在 COVID-19 的肾移植受者和透析患者中,ACEi/ARB 的使用或停药与死亡率之间无显著关联。