Mumba Jane Mwamba, Kasonka Lackson, Owiti Okola Basil, Andrew John, Lubeya Mwansa Ketty, Lukama Lufunda, Kasempa Charlotte, Msadabwe Susan C, Kalinda Chester
The University of Zambia, School of Medicine, Department of Obstetrics and Gynaecology, Nationalist Road, P/Box RWX1 50110, Ridgeway, Lusaka, Zambia.
Ndola Teaching Hospital, Department of Obstetrics and Gynaecology, Broadway Road, Postal Agency Ndola, Ndola, Zambia.
Gynecol Oncol Rep. 2021 May 13;37:100784. doi: 10.1016/j.gore.2021.100784. eCollection 2021 Aug.
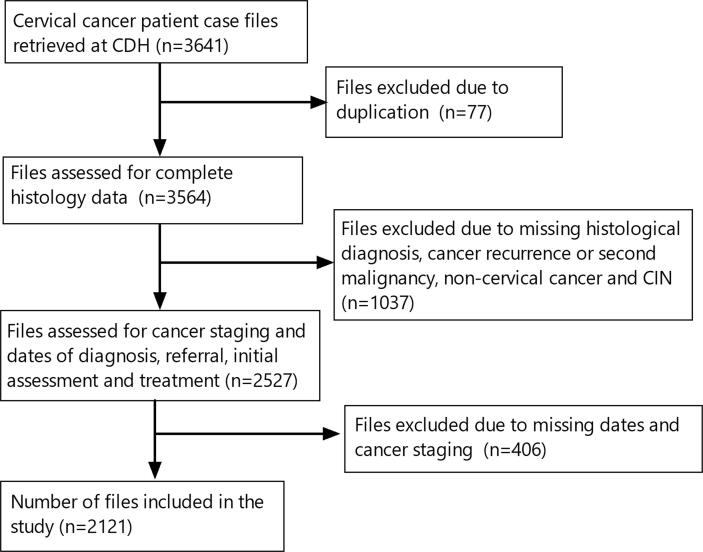
Expedited diagnostic processes for all suspected cervical cancer cases remain essential in the effort to improve clinical outcomes of the disease. However, in some developing countries like Zambia, there is paucity of data that assesses factors influencing diagnostic and treatment turnaround time (TAT) and other metrics vital for quality cancer care. We conducted a retrospective hospital-based study at the Cancer Diseases Hospital (CDH) for cervical cancer cases presenting to the facility between January 2014 and December 2018. Descriptive statistics were used to summarize demographic characteristics while a generalized linear model of the negative binomial was used to assess determinants of overall TAT. Our study included 2121 patient case files. The median age was 49 years (IQR: ±17) and most patients (n = 634, 31%) were aged between 41 and 50 years. The International Federation of Gynaecology and Obstetrics (FIGO) Cancer stage II (n = 941, 48%) was the most prevalent while stage IV (n = 103, 5.2%) was the least. The average diagnostic TAT in public laboratories was 1.48 (95%CI: 1.21-1.81) times longer than in private laboratories. Furthermore, referral delay was 55 days (IQR: 24-152) and the overall TAT (TAT) was 110 days (IQR: 62-204). The age of the patient, HIV status, stage of cancer and histological subtype did not influence TAT while marital status influenced TAT. The observed longer TAT may increase irreversible adverse health outcomes among cervical cancer patients. There is a need to improve cancer care in Zambia through improved health expenditure especially in public health facilities.
对所有疑似宫颈癌病例加快诊断流程,对于改善该疾病的临床治疗效果仍然至关重要。然而,在赞比亚等一些发展中国家,缺乏评估影响诊断和治疗周转时间(TAT)以及其他对优质癌症护理至关重要指标的因素的数据。我们在癌症疾病医院(CDH)开展了一项基于医院的回顾性研究,研究对象为2014年1月至2018年12月期间到该机构就诊的宫颈癌病例。采用描述性统计来总结人口统计学特征,同时使用负二项式广义线性模型来评估总体TAT的决定因素。我们的研究纳入了2121份患者病例档案。中位年龄为49岁(四分位距:±17),大多数患者(n = 634,31%)年龄在41至50岁之间。国际妇产科联合会(FIGO)癌症分期II期(n = 941,48%)最为常见,而IV期(n = 103,5.2%)最少见。公共实验室的平均诊断TAT比私人实验室长1.48倍(95%置信区间:1.21 - 1.81)。此外,转诊延迟为55天(四分位距:24 - 152),总体TAT为110天(四分位距:62 - 204)。患者年龄、艾滋病毒感染状况、癌症分期和组织学亚型不影响TAT,而婚姻状况影响TAT。观察到的较长TAT可能会增加宫颈癌患者不可逆转的不良健康结局。有必要通过增加卫生支出,特别是在公共卫生设施方面,来改善赞比亚的癌症护理。