Department of Colorectal Surgery, Magellan Centre, Haut-Leveque Hospital, University of Bordeaux, 33604 Pessac, France.
Département de Chirurgie Oncologique, ICM Val d'Aurelle, Montpellier, France.
BJS Open. 2021 May 7;5(3). doi: 10.1093/bjsopen/zrab043.
Local excision (LE) after chemoradiotherapy is a new option in low rectal cancer, but morbidity has never been compared prospectively with total mesorectal excision (TME). Early and late morbidity were compared in patients treated either by LE or TME after neoadjuvant chemoradiotherapy for rectal cancer.
This was a post-hoc analysis from a randomized trial. Patients with clinical T2/T3 low rectal cancer with good response to the chemoradiotherapy and having either LE, LE with eventual completion TME, or TME were considered. Early (1 month) and late (2 years) morbidities were compared between the three groups.
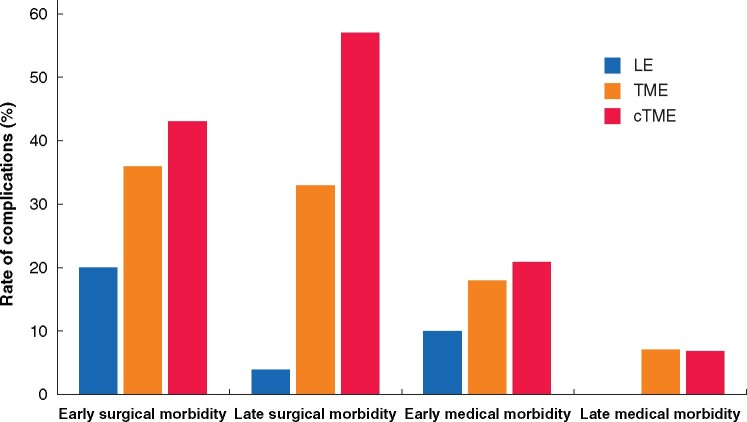
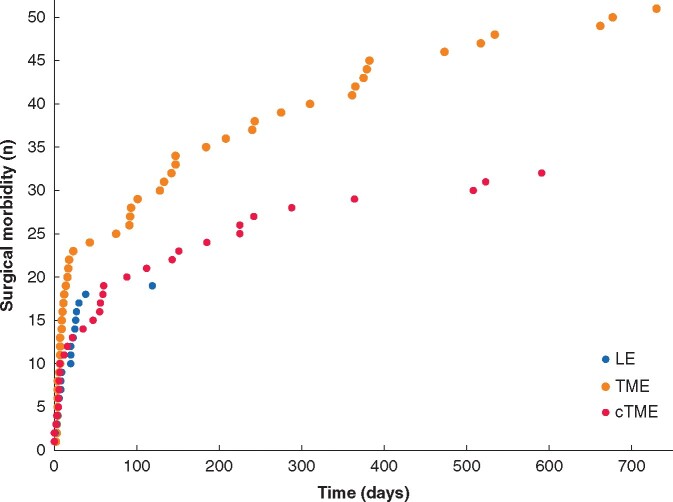
There were no deaths following surgery in any of the three groups. Early surgical morbidity (20 per cent LE versus 36 per cent TME versus 43 per cent completion TME, P = 0.025) and late surgical morbidity (4 per cent versus 33 per cent versus 57 per cent, P < 0.001) were significantly lower in the LE group than in the TME or the completion TME group. of LE, was associated with the lowest rate of early (10 versus 18 versus 21 per cent, P = 0.217) and late medical morbidities (0 versus 7 versus 7 per cent, P = 0.154), although this did not represent a significant difference between the groups. The severity of overall morbidity was significantly lower at 2 years after LE compared with TME or completion TME (4 versus 28 versus 43 per cent grade 3-5, P < 0.001).
The rate of surgical complications after neoadjuvant chemoradiotherapy in the LE group was half that of TME group at 1 month and 10 times lower at 2 years. LE is a safe approach for organ preservation and should be considered as an alternative to watch-and-wait in complete clinical responders and to TME in subcomplete responders.
新辅助放化疗后局部切除术(LE)是低位直肠癌的一种新选择,但发病率从未与全直肠系膜切除术(TME)进行前瞻性比较。本研究比较了新辅助放化疗后接受 LE 或 TME 治疗的直肠癌患者的早期和晚期发病率。
这是一项随机试验的事后分析。接受新辅助放化疗后临床 T2/T3 低位直肠癌且对放化疗反应良好的患者,接受 LE、LE 最终完成 TME 或 TME。比较三组之间的早期(1 个月)和晚期(2 年)发病率。
三组患者均无术后死亡。LE 组的早期手术发病率(20% vs. 36% TME vs. 43%完成 TME,P=0.025)和晚期手术发病率(4% vs. 33% vs. 57%,P<0.001)明显低于 TME 组或完成 TME 组。LE 组中,LE 组的早期(10% vs. 18% vs. 21%,P=0.217)和晚期医疗发病率(0% vs. 7% vs. 7%,P=0.154)也最低,尽管这三组之间没有显著差异。LE 组在 2 年时的整体发病率明显低于 TME 组或完成 TME 组(4% vs. 28% vs. 43%,3-5 级,P<0.001)。
LE 组在新辅助放化疗后 1 个月时的手术并发症发生率为 TME 组的一半,2 年后为 TME 组的十分之一。LE 是一种安全的器官保留方法,对于完全临床反应者应考虑作为观察等待的替代方法,对于部分反应者应考虑作为 TME 的替代方法。