Monaghan Anna M, Mulhern Maria S, McSorley Emeir M, Strain J J, Dyer Matthew, van Wijngaarden Edwin, Yeates Alison J
Nutrition Innovation Centre for Food and Health, Ulster University, Coleraine, Northern Ireland.
The Department of Community and Preventive Medicine, University of Rochester School of Medicine and Dentistry, Rochester, NY, USA.
Thyroid Res. 2021 Jun 7;14(1):14. doi: 10.1186/s13044-021-00105-1.
Mild to moderate iodine deficiency during pregnancy has been associated with adverse neurodevelopmental outcomes in offspring. Few research studies to date combine assessment of urinary iodine (UIC and/or ICr), biomarkers that best reflect dietary intake, with reported dietary intake of iodine rich foods in their assessment of iodine deficiency. Thus, a systematic review was conducted to incorporate both these important measures.
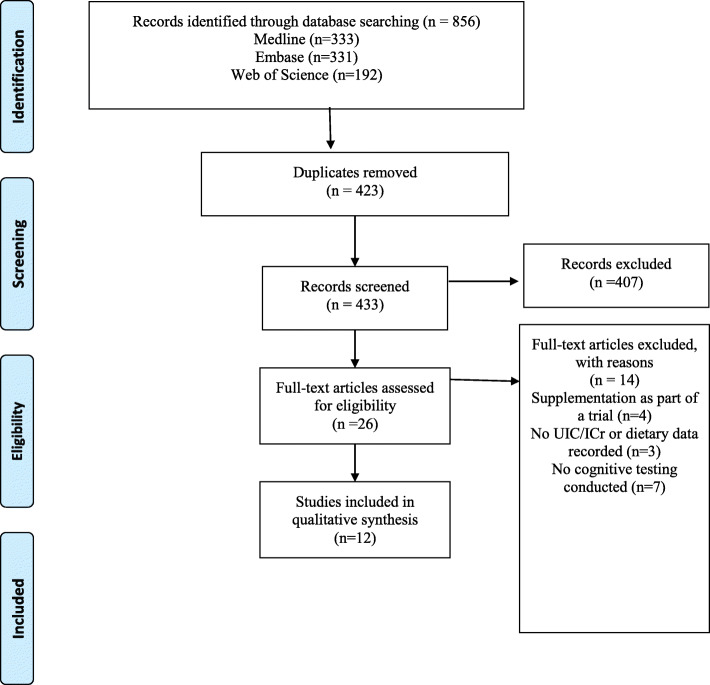
Using PRISMA guidelines, a comprehensive search was conducted in three electronic databases (EMBASE®, MedLine® and Web of Science®) from January 1970-March 2021. Quality assessment was undertaken using the Newcastle Ottawa Scale. Eligible studies included reported assessment of iodine status through urinary iodine (UIC and/or ICr) and/or dietary intake measures in pregnancy alongside neurodevelopmental outcomes measured in the children. Data extracted included study author, design, sample size, country, gestational age, child age at testing, cognitive tests, urinary iodine assessment (UIC in μg/L and/or ICr in μg/g), dietary iodine intake assessment and results of associations for the assessed cognitive outcomes.
Twelve studies were included with nine reporting women as mild-moderately iodine deficient based on World Health Organization (WHO) cut-offs for urinary iodine measurements < 150 μg/l, as the median UIC value in pregnant women. Only four of the nine studies reported a negative association with child cognitive outcomes based on deficient urinary iodine measurements. Five studies reported urinary iodine measurements and dietary intakes with four of these studies reporting a negative association of lower urinary iodine measurements and dietary iodine intakes with adverse offspring neurodevelopment. Milk was identified as the main dietary source of iodine in these studies.
The majority of studies classified pregnant women to be mild-moderately iodine deficient based on urinary iodine assessment (UIC and/or ICr) and/or dietary intakes, with subsequent offspring neurodevelopment implications identified. Although a considerable number of studies did not report an adverse association with neurodevelopmental outcomes, these findings are still supportive of ensuring adequate dietary iodine intakes and urinary iodine monitoring throughout pregnancy due to the important role iodine plays within foetal neurodevelopment. This review suggests that dietary intake data may indicate a stronger association with cognitive outcomes than urinary iodine measurements alone. The strength of this review distinguishes results based on cognitive outcome per urinary iodine assessment strategy (UIC and/or ICr) with dietary data. Future work is needed respecting the usefulness of urinary iodine assessment (UIC and/or ICr) as an indicator of deficiency whilst also taking account of dietary intakes.
孕期轻度至中度碘缺乏与后代不良神经发育结局有关。迄今为止,很少有研究在评估碘缺乏时,将最能反映饮食摄入量的尿碘(尿碘浓度和/或碘肌酐比值)评估与富含碘食物的报告饮食摄入量相结合。因此,进行了一项系统评价以纳入这两项重要指标。
采用PRISMA指南,于1970年1月至2021年3月在三个电子数据库(EMBASE®、MedLine®和Web of Science®)中进行了全面检索。使用纽卡斯尔渥太华量表进行质量评估。符合条件的研究包括报告通过尿碘(尿碘浓度和/或碘肌酐比值)和/或孕期饮食摄入量评估碘状态,以及对儿童进行的神经发育结局测量。提取的数据包括研究作者、设计、样本量、国家、孕周、测试时儿童年龄、认知测试、尿碘评估(尿碘浓度,μg/L和/或碘肌酐比值,μg/g)、饮食碘摄入量评估以及评估的认知结局的关联结果。
纳入了12项研究,其中9项报告称,根据世界卫生组织(WHO)尿碘测量值<150μg/l的临界值,孕妇为轻度至中度碘缺乏,这是孕妇尿碘浓度的中位数。在这9项研究中,只有4项报告称,基于尿碘测量值不足,与儿童认知结局呈负相关。5项研究报告了尿碘测量值和饮食摄入量,其中4项研究报告称,尿碘测量值和饮食碘摄入量较低与后代不良神经发育呈负相关。在这些研究中,牛奶被确定为碘的主要饮食来源。
大多数研究根据尿碘评估(尿碘浓度和/或碘肌酐比值)和/或饮食摄入量将孕妇分类为轻度至中度碘缺乏,并确定了对后代神经发育的影响。尽管相当多的研究没有报告与神经发育结局的不良关联,但由于碘在胎儿神经发育中起重要作用,这些发现仍支持在整个孕期确保充足的饮食碘摄入量和尿碘监测。本综述表明,饮食摄入量数据可能比单独的尿碘测量值与认知结局的关联更强。本综述的优势在于根据每种尿碘评估策略(尿碘浓度和/或碘肌酐比值)与饮食数据的认知结局区分结果。未来的工作需要考虑尿碘评估(尿碘浓度和/或碘肌酐比值)作为缺乏指标的有用性,同时也要考虑饮食摄入量。