School of Medicine.
Rollins School of Public Health, Emory University, Atlanta, Georgia.
Pediatrics. 2021 Jul;148(1). doi: 10.1542/peds.2020-027722. Epub 2021 Jun 7.
The progression of gender-expansive behavior to gender dysphoria and to gender-affirming hormonal treatment (GAHT) in children and adolescents is poorly understood.
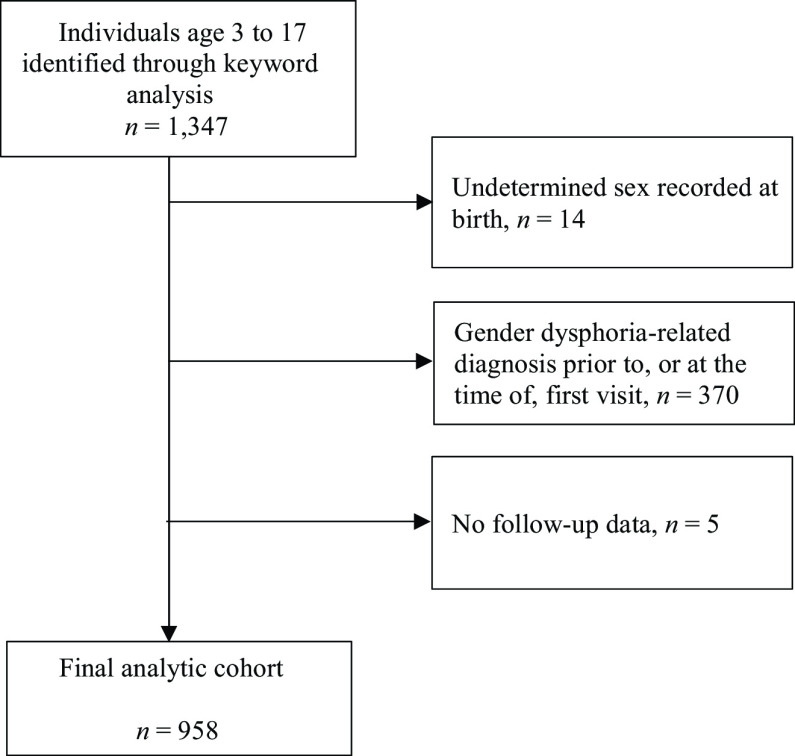
A cohort of 958 gender-diverse (GD) children and adolescents who did not have a gender dysphoria-related diagnosis (GDRD) or GAHT at index were identified. Rates of first GDRD and first GAHT prescription were compared across demographic groups.
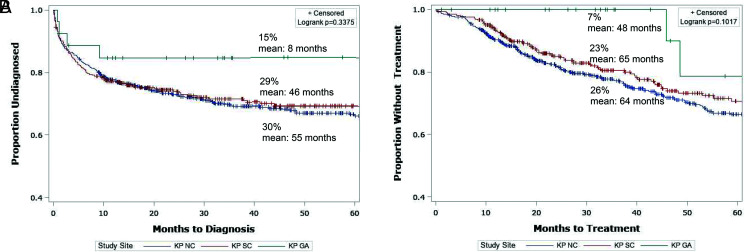
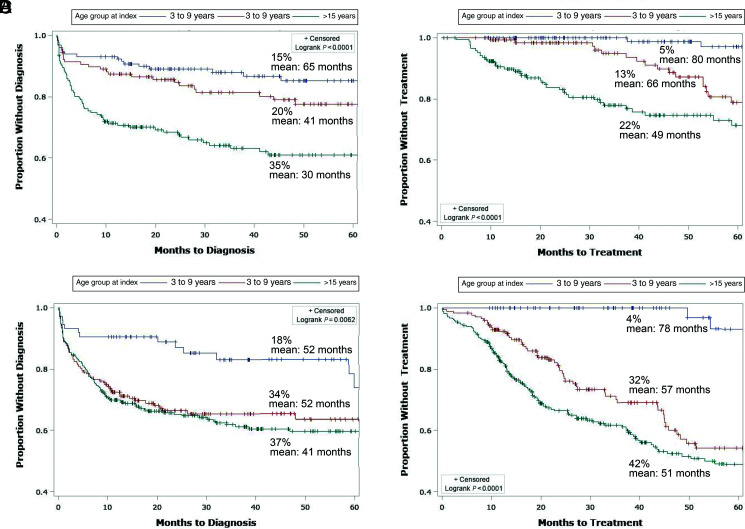
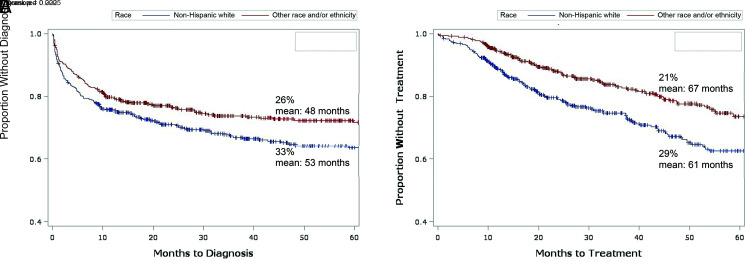
Overall, 29% of participants received a GDRD and 25% were prescribed GAHT during the average follow-up of 3.5 years (maximum 9 years). Compared with youth assigned male sex at birth, those assigned female sex at birth were more likely to receive a diagnosis and initiate GAHT with hazard ratio (95% confidence interval) estimates of 1.3 (1.0-1.7), and 2.5 (1.8-3.3), respectively. A progression to diagnosis was more common among those aged ≥15 years at initial presentation compared with those aged 10 to 14 years and those aged 3 to 9 years (37% vs 28% vs 16%, respectively). By using the youngest group as a reference, the adjusted hazard ratios (95% confidence interval) for a GDRD were 2.0 (1.3-3.0) for age 10 to 14 years and 2.7 (1.8-3.9) for age ≥15 years. Racial and ethnic minorities were less likely to receive a diagnosis or be prescribed GAHT.
This study characterized the progression of GD behavior in children and adolescents. Less than one-third of GD youth receive an eventual GDRD, and approximately one-quarter receive GAHT. Female sex at birth, older age of initial GD presentation to medical care, and non-Hispanic white race and ethnicity increased the likelihood of receiving diagnosis and treatment.
儿童和青少年的性别扩张行为向性别焦虑症和性别肯定激素治疗(GAHT)的进展知之甚少。
本研究确定了 958 名患有性别多样性(GD)但在指数时没有性别焦虑症相关诊断(GDRD)或 GAHT 的儿童和青少年队列。比较了不同人群中首次 GDRD 和首次 GAHT 处方的发生率。
总体而言,29%的参与者在平均 3.5 年(最长 9 年)的随访中接受了 GDRD 诊断,25%接受了 GAHT 处方。与出生时被分配为男性的青少年相比,出生时被分配为女性的青少年更有可能接受诊断并开始 GAHT,风险比(95%置信区间)估计值分别为 1.3(1.0-1.7)和 2.5(1.8-3.3)。与 10 至 14 岁和 3 至 9 岁的参与者相比,初次就诊时年龄≥15 岁的参与者向诊断的进展更为常见(分别为 37%、28%和 16%)。与年龄最小的组相比,年龄为 10 至 14 岁和年龄≥15 岁的青少年的 GDRD 调整后的风险比(95%置信区间)分别为 2.0(1.3-3.0)和 2.7(1.8-3.9)。少数族裔的青少年不太可能接受诊断或接受 GAHT 治疗。
本研究描述了儿童和青少年中 GD 行为的进展。不到三分之一的 GD 青少年最终会被诊断出患有 GDRD,大约四分之一的青少年会接受 GAHT 治疗。出生时为女性、初次就诊时年龄较大、非西班牙裔白人种族和民族增加了接受诊断和治疗的可能性。