Salahudeen Mohammed Saji, Duffull Stephen B, Nishtala Prasad S
School of Pharmacy, University of Otago, PO Box 56, Dunedin, 9054, New Zealand.
BMC Geriatr. 2015 Mar 25;15:31. doi: 10.1186/s12877-015-0029-9.
The cumulative effect of taking multiple medicines with anticholinergic properties termed as anticholinergic burden can adversely impact cognition, physical function and increase the risk of mortality. Expert opinion derived risk scales are routinely used in research and clinical practice to quantify anticholinergic burden. These scales rank the anticholinergic activity of medicines into four categories, ranging from no anticholinergic activity (= 0) to definite/high anticholinergic activity (= 3). The aim of this systematic review was to compare anticholinergic burden quantified by the anticholinergic risk scales and evaluate associations with adverse outcomes in older people.
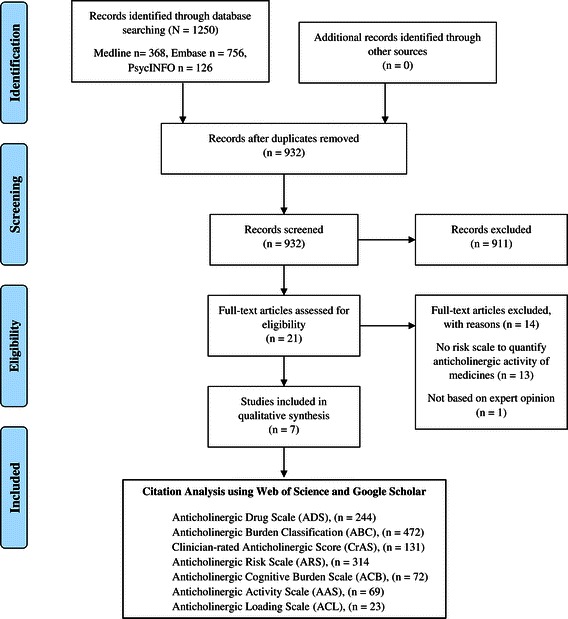
We conducted a literature search in Ovid MEDLINE, EMBASE and PsycINFO from 1984-2014 to identify expert opinion derived anticholinergic risk scales. In addition to this, a citation analysis was performed in Web of Science and Google Scholar to track prospective citing of references of selected articles for assessment of individual scales for adverse anticholinergic outcomes. The primary outcomes of interest were functional and cognitive outcomes associated with anticholinergic burden in older people. The critical appraisals of the included studies were performed by two independent reviewers and the data were extracted onto standardised forms.
The primary electronic literature search identified a total of 1250 records in the 3 different databases. On the basis of full-text analysis, we identified 7 expert-based anticholinergic rating scales that met the inclusion criteria. The rating of anticholinergic activity for medicines among these rating scales was inconsistent. For example, quetiapine was rated as having high anticholinergic activity in one scale (n = 1), moderate in another scale (n = 1) and low in two other scales (n = 2). Citation analysis of the individual scales showed that the Anticholinergic Cognitive Burden (ACB) scale was the most frequently validated expert based anticholinergic scale for adverse outcomes (N = 13).
In conclusion, there is not one standardised tool for measuring anticholinergic burden. Cohort studies have shown that higher anticholinergic burden is associated with negative brain effects, poorer cognitive and functional outcomes.
服用多种具有抗胆碱能特性的药物所产生的累积效应,即所谓的抗胆碱能负担,可能会对认知、身体功能产生不利影响,并增加死亡风险。在研究和临床实践中,通常使用基于专家意见的风险量表来量化抗胆碱能负担。这些量表将药物的抗胆碱能活性分为四类,从无抗胆碱能活性(=0)到明确/高抗胆碱能活性(=3)。本系统评价的目的是比较通过抗胆碱能风险量表量化的抗胆碱能负担,并评估其与老年人不良结局的关联。
我们在1984年至2014年期间对Ovid MEDLINE、EMBASE和PsycINFO进行了文献检索,以确定基于专家意见的抗胆碱能风险量表。除此之外,还在科学网和谷歌学术上进行了引文分析,以追踪所选文章参考文献的前瞻性引用情况,以评估个体量表的抗胆碱能不良结局。感兴趣的主要结局是与老年人抗胆碱能负担相关的功能和认知结局。纳入研究的批判性评价由两名独立的评审员进行,数据提取到标准化表格上。
初步电子文献检索在3个不同数据库中总共识别出1250条记录。基于全文分析,我们确定了7个符合纳入标准的基于专家的抗胆碱能评分量表。这些评分量表中药物的抗胆碱能活性评级不一致。例如,喹硫平在一个量表中被评为具有高抗胆碱能活性(n = 1),在另一个量表中为中度(n = 1),在另外两个量表中为低度(n = 2)。对各个量表的引文分析表明,抗胆碱能认知负担(ACB)量表是针对不良结局最常被验证的基于专家的抗胆碱能量表(N = 13)。
总之,目前尚无一种标准化的工具来测量抗胆碱能负担。队列研究表明,较高的抗胆碱能负担与负面的脑部影响、较差的认知和功能结局相关。