Shoklo Malaria Research Unit, Mahidol-Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Mae Sot, Thailand.
Centre for Tropical Medicine and Global Health, Nuffield Department of Medicine, University of Oxford, Oxford, UK.
BMC Med. 2021 Jun 10;19(1):132. doi: 10.1186/s12916-021-02002-8.
Artemisinin and artemisinin-based combination therapy (ACT) partner drug resistance in Plasmodium falciparum have spread across the Greater Mekong Subregion compromising antimalarial treatment. The current 3-day artemether-lumefantrine regimen has been associated with high treatment failure rates in pregnant women. Although ACTs are recommended for treating Plasmodium vivax malaria, no clinical trials in pregnancy have been reported.
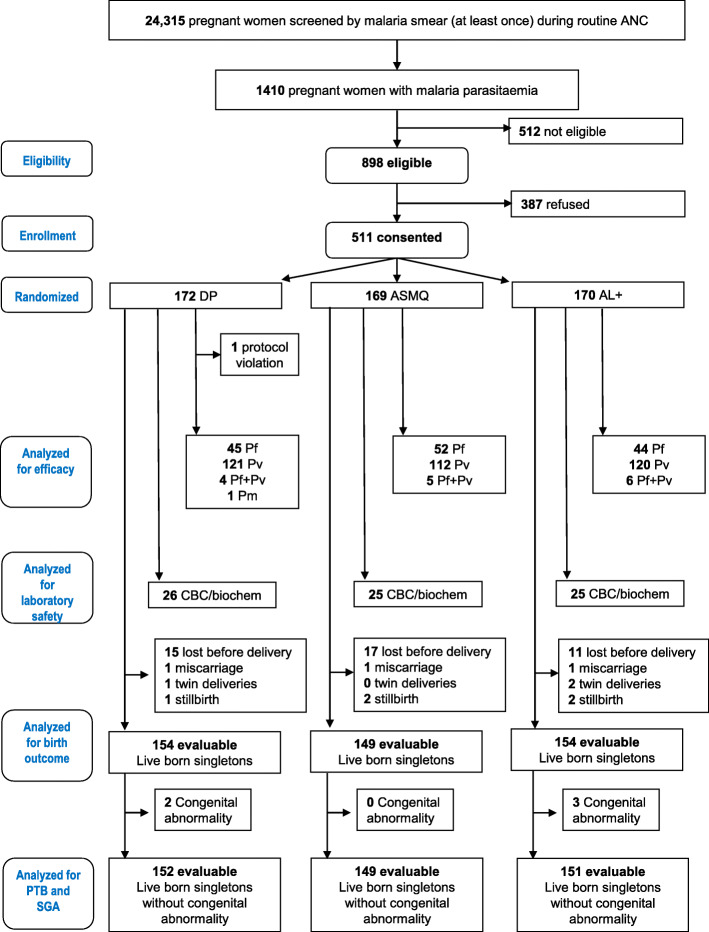
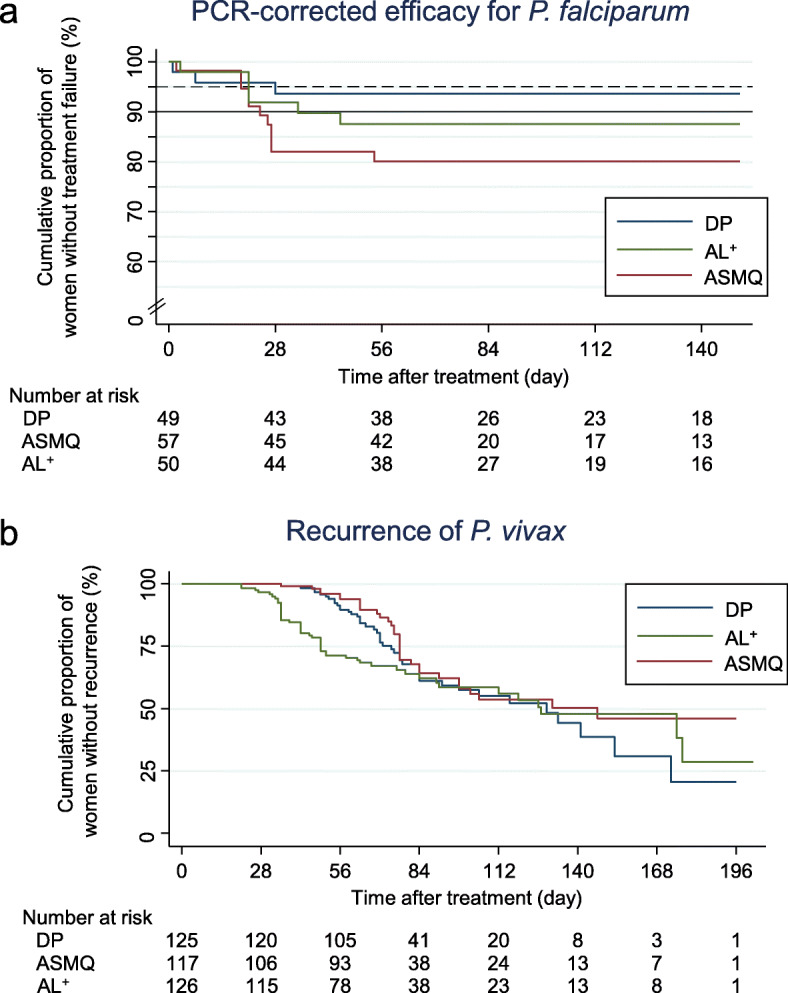
Pregnant women with uncomplicated malaria on the Thailand-Myanmar border participated in an open-label randomized controlled trial comparing dihydroartemisinin-piperaquine (DP), artesunate-mefloquine (ASMQ) and a 4-day artemether-lumefantrine regimen (AL). The primary endpoint for P. falciparum infections was the PCR-corrected cure rate and for P. vivax infections was recurrent parasitaemia, before delivery or day 63, whichever was longer, assessed by Kaplan-Meier estimate.
Between February 2010 and August 2016, 511 pregnant women with malaria (353 P. vivax, 142 P. falciparum, 15 co-infections, 1 Plasmodium malariae) were randomized to either DP (n=170), ASMQ (n=169) or AL (n=172) treatments. Successful malaria elimination efforts in the region resulted in premature termination of the trial. The majority of women had recurrent malaria (mainly P. vivax relapses, which are not prevented by these treatments). Recurrence-free proportions (95% confidence interval [95% CI]) for vivax malaria were 20.6% (5.1-43.4) for DP (n=125), 46.0% (30.9-60.0) for ASMQ (n=117) and 28.7% (10.0-50.8) for AL (n=126). DP and ASMQ provided longer recurrence-free intervals. PCR-corrected cure rates (95% CI) for falciparum malaria were 93.7% (81.6-97.9) for DP (n=49), 79.6% (66.1-88.1) for AMSQ (n=55) and 87.5% (74.3-94.2) for AL (n=50). Overall 65% (85/130) of P. falciparum infections had Pfkelch13 propeller mutations which increased over time and recrudescence occurred almost exclusively in them; risk ratio 9.42 (95% CI 1.30-68.29). Among the women with falciparum malaria, 24.0% (95% CI 16.8-33.6) had P. vivax parasitaemia within 4 months. Nausea, vomiting, dizziness and sleep disturbance were more frequent with ASMQ. Miscarriage, small-for-gestational-age and preterm birth did not differ significantly among the treatment groups, including first trimester exposures (n=46).
DP was well tolerated and safe, and was the only drug providing satisfactory efficacy for P. falciparum-infected pregnant woman in this area of widespread artemisinin resistance. Vivax malaria recurrences are very common and warrant chloroquine prophylaxis after antimalarial treatment in this area.
ClinicalTrials.gov identifier NCT01054248 , registered on 22 January 2010.
青蒿素及其复方疗法(ACT)的抗疟药物在恶性疟原虫中的耐药性已经在大湄公河次区域蔓延,这影响了抗疟治疗。目前使用的 3 天青蒿琥酯-咯萘啶疗法在孕妇中与高治疗失败率相关。尽管 ACT 被推荐用于治疗间日疟原虫疟疾,但在妊娠期间尚未报告有临床试验。
在泰国和缅甸边境地区患有无并发症疟疾的孕妇参与了一项开放性随机对照试验,比较双氢青蒿素-哌喹(DP)、青蒿琥酯-甲氟喹(ASMQ)和 4 天青蒿琥酯-咯萘啶疗法(AL)。主要终点为 PCR 校正的治愈率,对于间日疟原虫感染为复发性寄生虫血症,在分娩前或第 63 天(以较长者为准)进行评估,采用 Kaplan-Meier 估计。
2010 年 2 月至 2016 年 8 月,511 名患有疟疾的孕妇(353 例间日疟原虫、142 例恶性疟原虫、15 例混合感染、1 例恶性疟原虫)被随机分配至 DP(n=170)、ASMQ(n=169)或 AL(n=172)治疗组。该地区成功的疟疾消除工作导致试验提前终止。大多数妇女出现疟疾复发(主要是间日疟原虫复发,这些治疗方法无法预防)。间日疟原虫无复发生存率(95%置信区间[95%CI])为 DP(n=125)组 20.6%(5.1-43.4)、ASMQ(n=117)组 46.0%(30.9-60.0)和 AL(n=126)组 28.7%(10.0-50.8)。DP 和 ASMQ 提供了更长的无复发生存期。恶性疟原虫感染的 PCR 校正治愈率(95%CI)为 DP(n=49)组 93.7%(81.6-97.9)、ASMQ(n=55)组 79.6%(66.1-88.1)和 AL(n=50)组 87.5%(74.3-94.2)。总的来说,65%(85/130)的恶性疟原虫感染有 Pfkelch13 螺旋桨突变,这些突变随着时间的推移而增加,复燃几乎只发生在这些突变中;风险比 9.42(95%CI 1.30-68.29)。在患有恶性疟原虫感染的妇女中,24.0%(95%CI 16.8-33.6)在 4 个月内出现间日疟原虫寄生虫血症。ASMQ 组更常见恶心、呕吐、头晕和睡眠障碍。不良妊娠结局,包括小胎龄儿和早产,在各组之间没有显著差异,包括第一孕期暴露(n=46)。
DP 耐受性良好且安全,是该地区广泛存在青蒿素耐药性的孕妇中唯一能有效治疗恶性疟原虫感染的药物。间日疟原虫复发非常常见,在该地区抗疟治疗后需要氯喹预防。
ClinicalTrials.gov 标识符 NCT01054248,于 2010 年 1 月 22 日注册。