Limbada Mohammed, Zijlstra Geiske, Macleod David, Ayles Helen, Fidler Sarah
Zambart House, PO Box 50697, UNZA-Ridgeway Campus, Lusaka, Zambia.
Imperial College London, London, UK.
BMC Public Health. 2021 Jun 10;21(1):1110. doi: 10.1186/s12889-021-11053-8.
Alternative models for sustainable antiretroviral treatment (ART) delivery are necessary to meet the increasing demand to maintain population-wide ART for all people living with HIV (PLHIV) in sub-Saharan Africa. We undertook a review of published literature comparing health facility-based care (HFBC) with non-health facility based care (nHFBC) models of ART delivery in terms of health outcomes; viral suppression, loss to follow-up, retention and mortality.
We conducted a systematic search of Medline, Embase and Global Health databases from 2010 onwards. UNAIDS reports, WHO guidelines and abstracts from conferences were reviewed. All studies measuring at least one of the following outcomes, viral load suppression, loss-to-follow-up (LTFU) and mortality were included. Data were extracted, and a descriptive analysis was performed. Risk of bias assessment was done for all studies. Pooled estimates of the risk difference (for viral suppression) and hazard ratio (for mortality) were made using random-effects meta-analysis.
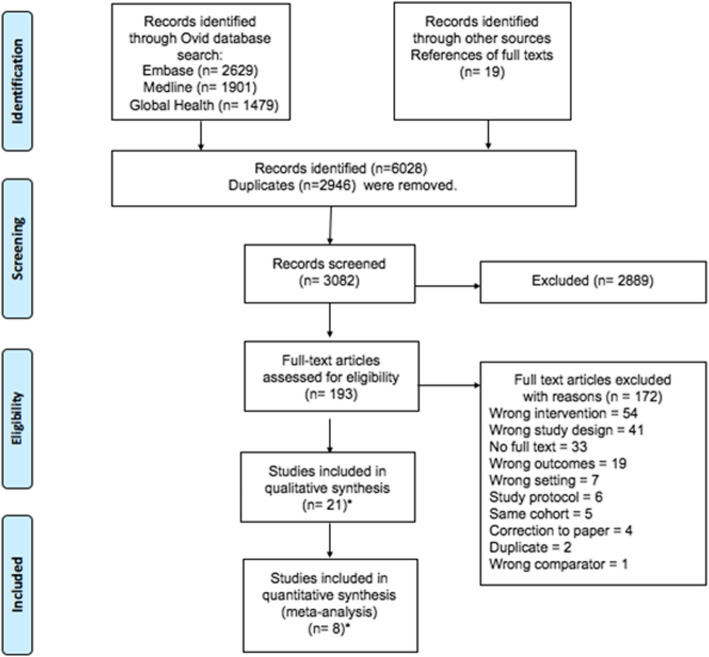
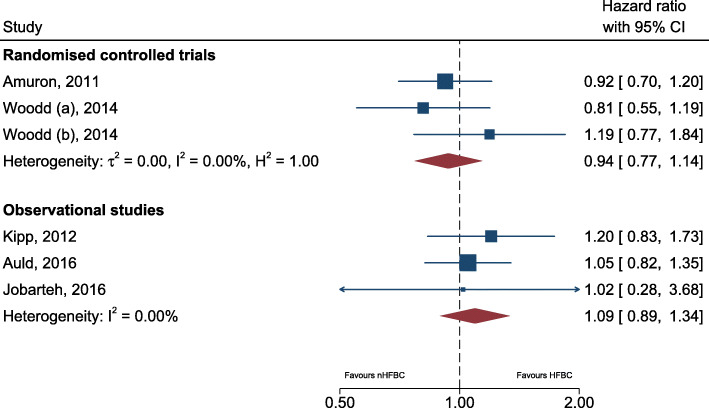
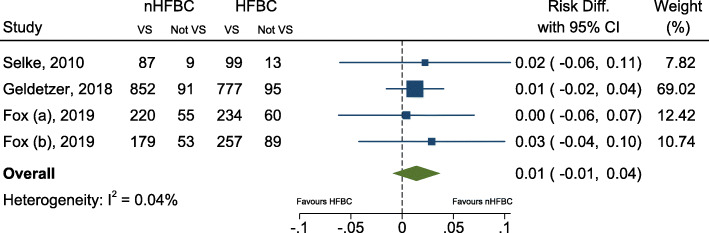
Of 3082 non-duplicate records, 193 were eligible for full text screening of which 21 published papers met the criteria for inclusion. The pooled risk difference of viral load suppression amongst 4 RCTs showed no evidence of a difference in viral suppression (VS) between nHFBC and HFBC with an overall estimated risk difference of 1% [95% CI -1, 4%]. The pooled hazard ratio of mortality amongst 2 RCTs and 4 observational cohort studies showed no evidence of a difference in mortality between nHFBC and HFBC with an overall estimated hazard ratio of 1.01 [95% CI 0.88, 1.16]. Fifteen studies contained data on LTFU and 13 studies on retention. Although no formal quantitative analysis was performed on these outcomes due to the very different definitions between papers, it was observed that the outcomes appeared similar between HFBC and nHFBC.
Review of current literature demonstrates comparable outcomes for nHFBC compared to HFBC ART delivery programmes in terms of viral suppression, retention and mortality.
CRD42018088194 .
为满足撒哈拉以南非洲地区所有艾滋病毒感染者(PLHIV)维持全民抗逆转录病毒治疗(ART)的需求不断增加,有必要采用可持续的ART提供替代模式。我们对已发表的文献进行了综述,比较了基于医疗机构的护理(HFBC)和非基于医疗机构的护理(nHFBC)两种ART提供模式在健康结局方面的差异,包括病毒抑制、失访、留存率和死亡率。
我们对2010年起的Medline、Embase和全球健康数据库进行了系统检索。审查了联合国艾滋病规划署的报告、世界卫生组织的指南以及会议摘要。纳入所有测量以下至少一项结局的研究:病毒载量抑制、失访(LTFU)和死亡率。提取数据并进行描述性分析。对所有研究进行偏倚风险评估。使用随机效应荟萃分析对风险差异(针对病毒抑制)和风险比(针对死亡率)进行汇总估计。
在3082条非重复记录中,193条符合全文筛选条件,其中21篇已发表论文符合纳入标准。4项随机对照试验中病毒载量抑制的汇总风险差异显示,nHFBC和HFBC之间在病毒抑制(VS)方面没有差异的证据,总体估计风险差异为1%[95%置信区间 -1, 4%]。2项随机对照试验和4项观察性队列研究中死亡率的汇总风险比显示,nHFBC和HFBC之间在死亡率方面没有差异的证据,总体估计风险比为1.01[95%置信区间0.88, 1.16]。15项研究包含LTFU数据,13项研究包含留存率数据。尽管由于各论文之间定义差异很大,未对这些结局进行正式的定量分析,但观察到HFBC和nHFBC之间的结局似乎相似。
对当前文献的综述表明,与HFBC的ART提供项目相比,nHFBC在病毒抑制、留存率和死亡率方面的结局相当。
PROSPERO编号:CRD42018088194 。