Institute of Diagnostic and Interventional Radiology, University Hospital Zurich, University of Zurich, Raemistrasse 100, 8091, Zurich, Switzerland.
Institute for Biomedical Engineering, University and ETH Zurich, Gloriastrasse 35, 8092, Zurich, Switzerland.
Sci Rep. 2021 Jun 11;11(1):12376. doi: 10.1038/s41598-021-90283-7.
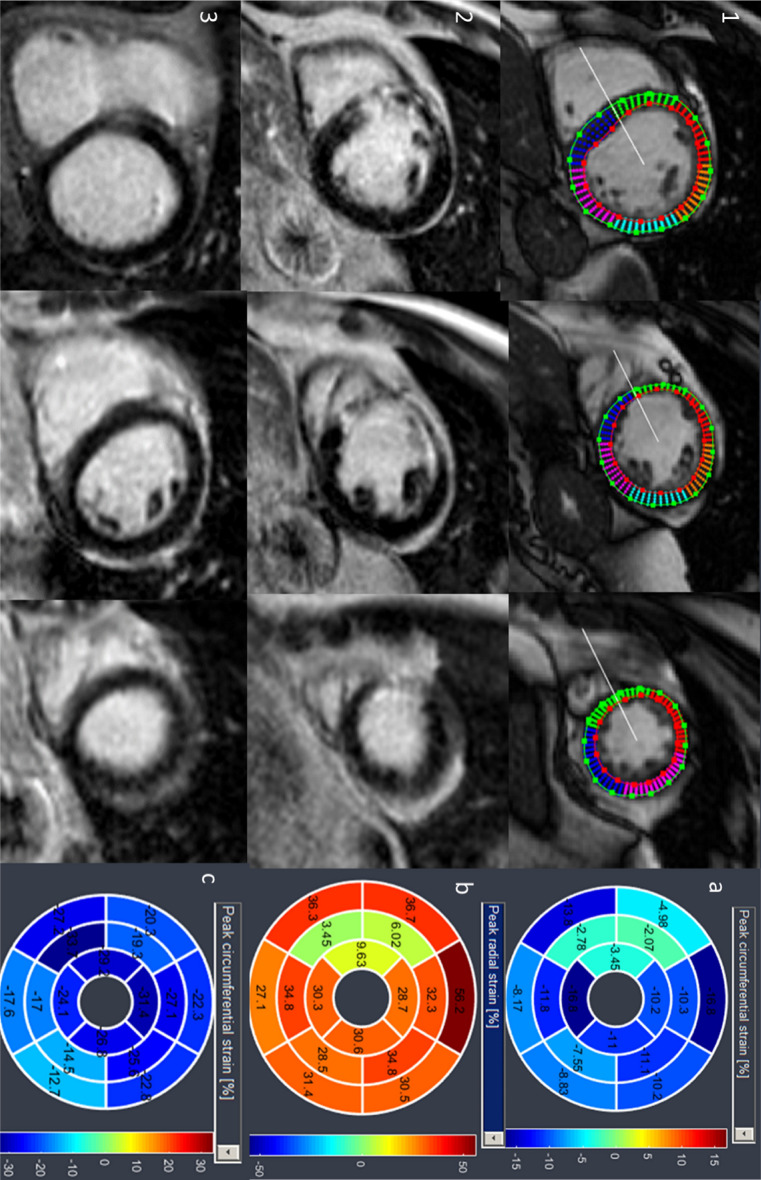
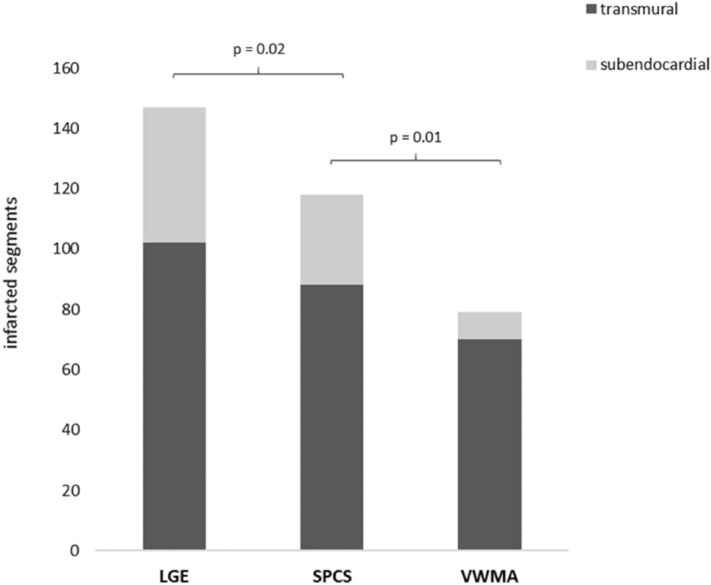
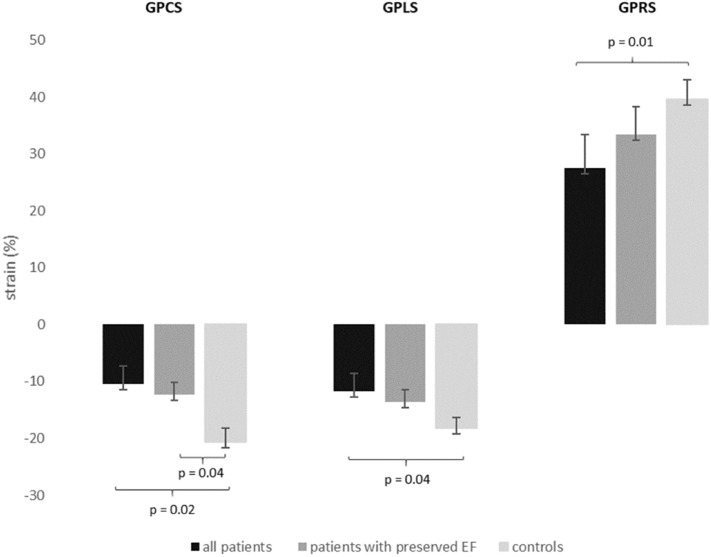
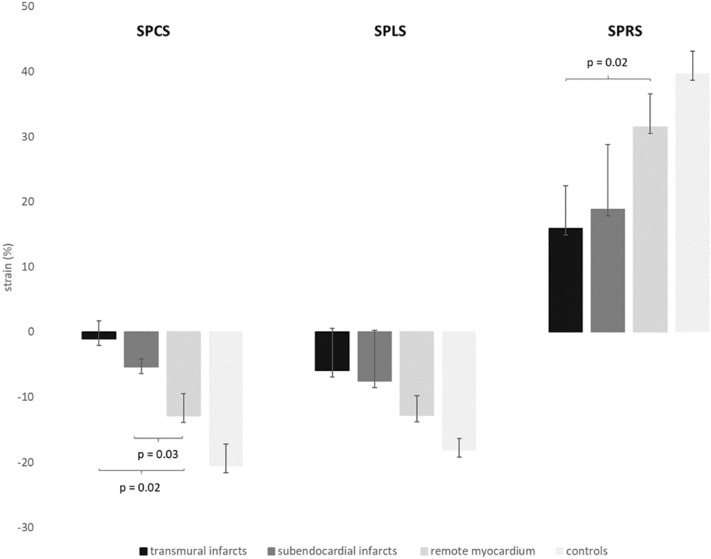
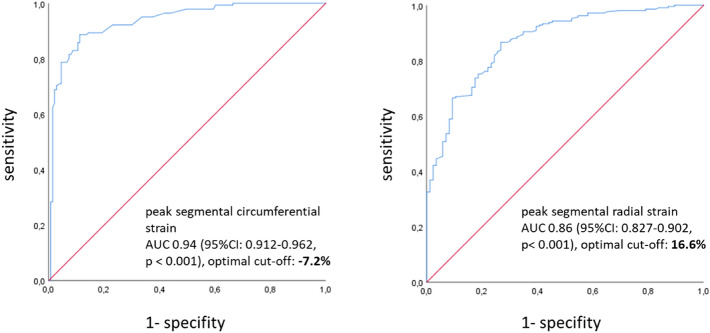
Cardiac magnetic resonance imaging (MRI) with late gadolinium enhancement (LGE) is considered the gold standard for scar detection after myocardial infarction. In times of increasing skepticism about gadolinium depositions in brain tissue and contraindications of gadolinium administration in some patient groups, tissue strain-based techniques for detecting ischemic scars should be further developed as part of clinical protocols. Therefore, the objective of the present work was to investigate whether segmental strain is noticeably affected in chronic infarcts and thus can be potentially used for infarct detection based on routinely acquired non-contrast cine images in patients with known coronary artery disease (CAD). Forty-six patients with known CAD and chronic scars in LGE images (5 female, mean age 52 ± 19 years) and 24 gender- and age-matched controls with normal cardiac MRI (2 female, mean age 47 ± 13 years) were retrospectively enrolled. Global (global peak circumferential [GPCS], global peak longitudinal [GPLS], global peak radial strain [GPRS]) and segmental (segmental peak circumferential [SPCS], segmental peak longitudinal [SPLS], segmental peak radial strain [SPRS]) strain parameters were calculated from standard non-contrast balanced SSFP cine sequences using commercially available software (Segment CMR, Medviso, Sweden). Visual wall motion assessment of short axis cine images as well as segmental circumferential strain calculations (endo-/epicardially contoured short axis cine and resulting polar plot strain map) of every patient and control were presented in random order to two independent blinded readers, which should localize potentially infarcted segments in those datasets blinded to LGE images and patient information. Global strain values were impaired in patients compared to controls (GPCS p = 0.02; GPLS p = 0.04; GPRS p = 0.01). Patients with preserved ejection fraction showed also impeded GPCS compared to healthy individuals (p = 0.04). In patients, mean SPCS was significantly impaired in subendocardially (- 5.4% ± 2) and in transmurally infarcted segments (- 1.2% ± 3) compared to remote myocardium (- 12.9% ± 3, p = 0.02 and 0.03, respectively). ROC analysis revealed an optimal cut-off value for SPCS for discriminating infarcted from remote myocardium of - 7.2% with a sensitivity of 89.4% and specificity of 85.7%. Mean SPRS was impeded in transmurally infarcted segments (15.9% ± 6) compared to SPRS of remote myocardium (31.4% ± 5; p = 0.02). The optimal cut-off value for SPRS for discriminating scar tissue from remote myocardium was 16.6% with a sensitivity of 83.3% and specificity of 76.5%. 80.3% of all in LGE infarcted segments (118/147) were correctly localized in segmental circumferential strain calculations based on non-contrast cine images compared to 53.7% (79/147) of infarcted segments detected by visual wall motion assessment (p > 0.01). Global strain parameters are impaired in patients with chronic infarcts compared to controls. Mean SPCS and SPRS in scar tissue is impeded compared to remote myocardium in infarcts patients. Blinded to LGE images, two readers correctly localized 80% of infarcted segments in segmental circumferential strain calculations based on non-contrast cine images, in contrast to only 54% of infarcted segments detected due to wall motion abnormalities in visual wall motion assessment. Analysis of segmental circumferential strain shows a promising method for detection of chronic scars in routinely acquired, non-contrast cine images for patients who cannot receive or decline gadolinium.
心脏磁共振成像(MRI)结合晚期钆增强(LGE)被认为是心肌梗死后检测疤痕的金标准。在人们对脑组织中钆沉积越来越怀疑以及某些患者群体中钆给药存在禁忌症的情况下,应该进一步开发基于组织应变的技术来检测缺血性疤痕,作为临床方案的一部分。因此,本研究的目的是探讨节段应变是否在慢性梗死中明显受到影响,从而可以潜在地用于在已知冠心病(CAD)的患者中基于常规采集的非对比电影图像进行梗死检测。回顾性纳入 46 名已知 CAD 且 LGE 图像中有慢性疤痕的患者(5 名女性,平均年龄 52 ± 19 岁)和 24 名性别和年龄匹配的无心脏 MRI 异常的对照者(2 名女性,平均年龄 47 ± 13 岁)。使用商业软件(Segment CMR,Medviso,瑞典)从标准非对比平衡 SSFP 电影序列中计算全局(全局峰值周向应变[GPCS]、全局峰值纵向应变[GPLS]、全局峰值径向应变[GPRS])和节段(节段峰值周向应变[SPCS]、节段峰值纵向应变[SPLS]、节段峰值径向应变[SPRS])应变参数。每位患者和对照者的短轴电影图像的视觉壁运动评估以及节段圆周应变计算(心内膜/心外膜勾画的短轴电影和由此产生的极坐标应变图)以随机顺序呈现给两名独立的盲法读者,读者应在不知道 LGE 图像和患者信息的情况下定位这些数据集潜在的梗死节段。与对照组相比,患者的整体应变值受损(GPCS p = 0.02;GPLS p = 0.04;GPRS p = 0.01)。与健康个体相比,射血分数保留的患者的 GPCS 也受损(p = 0.04)。在患者中,与远程心肌相比,心内膜下(-5.4% ± 2)和透壁性梗死节段(-1.2% ± 3)的平均 SPCS 明显受损(p = 0.02 和 0.03)。ROC 分析显示,用于区分梗死和远程心肌的 SPCS 最佳截断值为-7.2%,其敏感性为 89.4%,特异性为 85.7%。与远程心肌相比,透壁性梗死节段的平均 SPRS 受损(15.9% ± 6)(p = 0.02)。用于区分疤痕组织和远程心肌的 SPRS 最佳截断值为 16.6%,其敏感性为 83.3%,特异性为 76.5%。与视觉壁运动评估(53.7%[79/147])相比,基于非对比电影图像的节段圆周应变计算正确定位 LGE 梗死节段的 80.3%(118/147)(p>0.01)。与对照组相比,慢性梗死患者的整体应变参数受损。与梗死患者的远程心肌相比,疤痕组织中的平均 SPCS 和 SPRS 受损。在不知道 LGE 图像的情况下,两名读者在基于非对比电影图像的节段圆周应变计算中正确定位了 80%的梗死节段,而在视觉壁运动评估中,由于壁运动异常,仅能检测到 54%的梗死节段(p>0.01)。节段圆周应变分析显示,在不能接受或拒绝钆给药的患者中,在常规采集的非对比电影图像中检测慢性疤痕是一种很有前途的方法。