Stern M D, Silverman H S, Houser S R, Josephson R A, Capogrossi M C, Nichols C G, Lederer W J, Lakatta E G
Gerontology Research Center, National Institute on Aging, Baltimore, MD 21224.
Proc Natl Acad Sci U S A. 1988 Sep;85(18):6954-8. doi: 10.1073/pnas.85.18.6954.
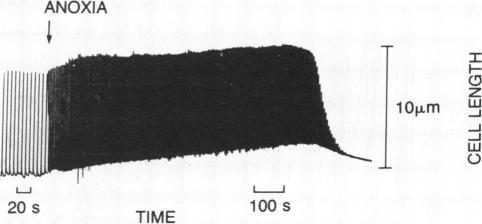
Anoxia of the heart causes failure of contraction before any irreversible injury occurs; the mechanism by which anoxia blocks cardiac excitation-contraction coupling is unknown. Studies in whole muscle are confounded by heterogeneity; however, achieving the low oxygen tensions required to study anoxia in a single myocyte during electrophysiological recording has been a barrier in experimental design. Guided by calculations of oxygen transport, we developed a system to insulate myocytes in an open dish from oxygen by a laminar counterflowing argon column, permitting free access to the cell by microelectrodes while maintaining a PO2 less than 0.02 torr (1 torr = 133 Pa). In the absence of glucose, the amplitude of stimulated contraction of anoxic ventricular myocytes fell to zero over 2 min after a lag period attributable to the consumption of endogenous glycogen. The cytosolic calcium concentration transient, measured by indo-1 fluorescence, fell to zero simultaneously with contraction. After the twitch had failed, microinjection of caffeine around the cell still caused a large calcium release and contraction, indicating that sarcoplasmic reticular calcium stores were not depleted. Twitch failure was accompanied by shortening and then failure of the action potential; under voltage clamp, large outward currents, reversing at the resting potential, developed during contractile failure. After failure of action potential-mediated contraction, voltage-clamp depolarization, with a large command voltage to compensate for the series-resistance error due to outward currents, restored normal twitch contraction. We conclude that anoxic contractile failure in the rat myocyte is due to alteration of the action potential and the distal pathways of excitation-contraction coupling remain essentially intact.
心脏缺氧在任何不可逆损伤发生之前就会导致收缩功能衰竭;缺氧阻断心脏兴奋 - 收缩偶联的机制尚不清楚。对整块肌肉的研究因异质性而受到干扰;然而,在电生理记录过程中,要在单个心肌细胞中达到研究缺氧所需的低氧张力一直是实验设计中的一个障碍。在氧运输计算的指导下,我们开发了一种系统,通过层流反向流动的氩气柱将培养皿中的心肌细胞与氧气隔绝,在保持氧分压低于0.02托(1托 = 133帕斯卡)的同时,允许微电极自由接触细胞。在没有葡萄糖的情况下,缺氧心室肌细胞受刺激收缩的幅度在经过一段因内源性糖原消耗导致的延迟期后,在2分钟内降至零。通过indo - 1荧光测量的胞质钙浓度瞬变与收缩同时降至零。抽搐失败后,在细胞周围微量注射咖啡因仍会引起大量钙释放和收缩,表明肌浆网钙储备未耗尽。抽搐失败伴随着动作电位缩短然后消失;在电压钳制下,在收缩失败期间出现了大的外向电流,该电流在静息电位处反转。动作电位介导的收缩失败后,通过大的指令电压进行电压钳制去极化以补偿由于外向电流引起的串联电阻误差,可恢复正常的抽搐收缩。我们得出结论,大鼠心肌细胞中的缺氧收缩失败是由于动作电位的改变,而兴奋 - 收缩偶联的远端途径基本保持完整。